Tagged: Infectious diseases
Why a Rare Ebola Variant is Currently Outpacing Global Science: 5 Critical Takeaways
Introduction: The Ghost in the System
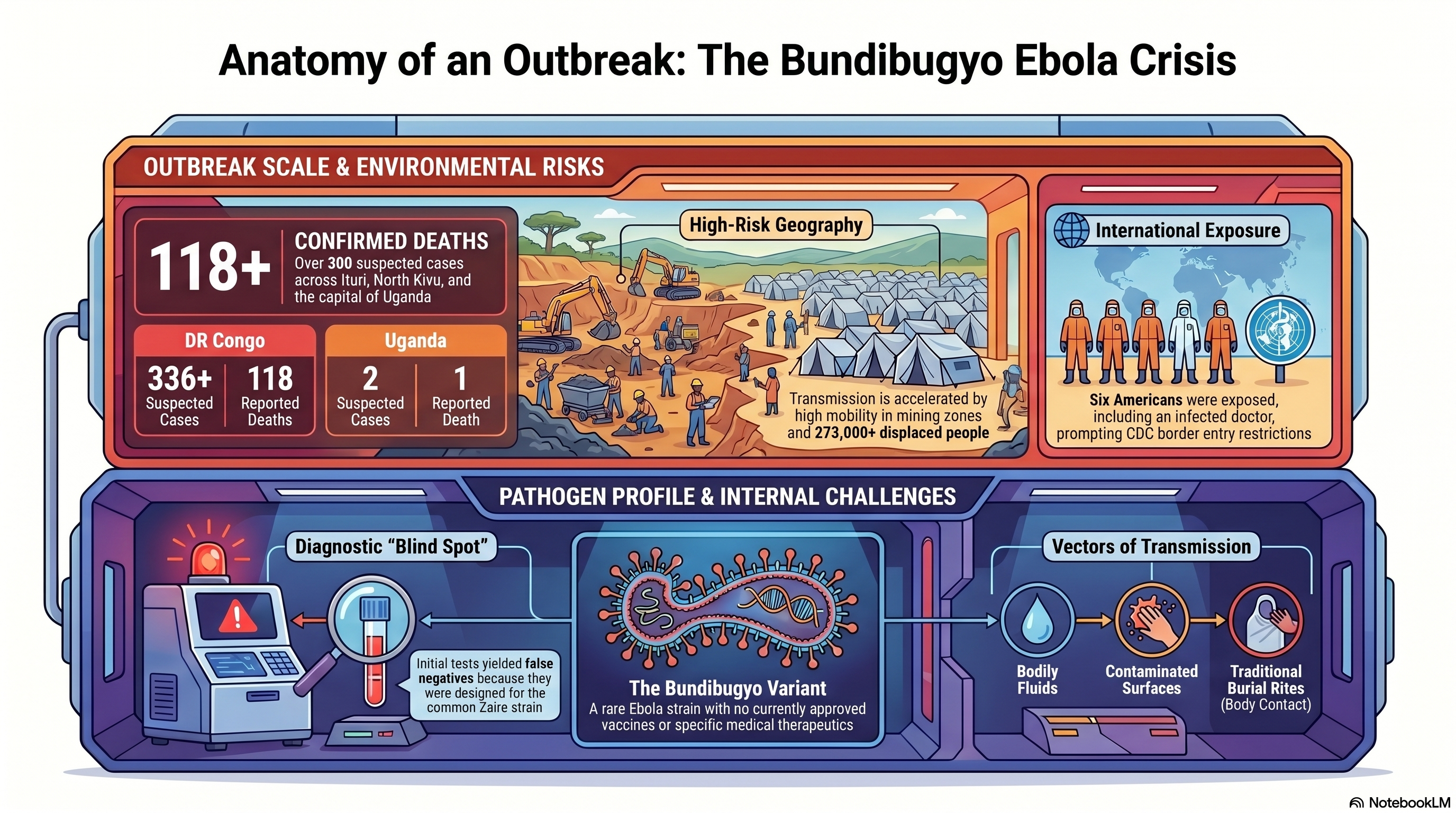
In the modern landscape of high-speed digital surveillance and automated biosensors, we have allowed ourselves to believe that a pathogen can no longer move in total silence. That illusion shattered in late April 2026. In the Ituri province of the Democratic Republic of Congo (DRC), a “mystery” illness began carving a path through remote mining communities, eventually escalating into a crisis that has now claimed 118 lives across the DRC and Uganda.
The culprit is the Bundibugyo Ebola virus—a rare, virulent strain that has appeared only three times since its discovery in 1976. This is not a simple resurgence of a familiar foe; it is a clinical and logistical outlier. While global health systems were calibrated for the common Zaire strain, Bundibugyo exploited our systemic blind spots, outpacing scientific intervention before the world even realized a race had begun.
1. The “Invisible” Strain: A Failure of Presumptive Testing
The Bundibugyo variant gained a lethal foothold because the global surveillance system is currently blind to its own gaps. When patients first presented with fever, muscle pain, and vomiting in late April, health officials deployed standard rapid field tests. These tests, however, were optimized for the Zaire strain. Because the symptoms mimicked other endemic tropical diseases, the negative results for Zaire Ebola provided a false sense of security that allowed the virus to circulate unhindered for weeks.
The diagnostic timeline reveals a catastrophic delay. It was not until May 14 that Ebola of any kind was confirmed, and only on May 15 was the Bundibugyo strain identified. By then, the virus had already infiltrated urban hubs like Bunia and crossed international borders.
“Because early tests looked for the wrong strain of Ebola, we got false negatives and lost weeks of response time,” says Matthew M. Kavanagh, director of the Georgetown University Center for Global Health Policy and Politics. “We are playing catch-up against a very dangerous pathogen.”
2. A Medical Blank Slate: The Zero-Vaccine Reality
The most harrowing reality for science communicators and health officials is the total absence of a medical safety net. Despite the massive research investment following the 2014-2016 West African epidemic, there are currently zero approved vaccines or therapeutics for the Bundibugyo strain.
Public health leaders are now forced into what Africa CDC Director General Dr. Jean Kaseya calls “panic mode.” While an experimental vaccine candidate exists, its data is a coin-flip: it has shown approximately 50% efficacy in primates, but its impact on humans is entirely unknown. For those on the ground, a 50% efficacy rate is a communication nightmare—it offers a glimmer of hope while simultaneously failing to provide the decisive protection needed to break the chain of transmission. This lack of tools is further complicated by cultural friction; Kaseya has issued urgent warnings regarding funeral practices, as traditional body-washing remains a primary driver of infection in the absence of pharmaceutical interventions.
3. The Frontline Vulnerability: High-Stakes Exposure
The surveillance gap has already exacted a heavy toll on the global and local medical community. In the provincial capital of Bunia, one American doctor has been laboratory-confirmed as an Ebola case. Furthermore, at least six other Americans have been exposed, prompting the U.S. CDC to coordinate their withdrawal and potential quarantine.
However, the deadliest impact remains local. In the Mongbwalu mining area, at least four healthcare workers died before the virus was even identified. This highlights the extreme risk of nosocomial (hospital-acquired) transmission. When clinics lack specialized Personal Protective Equipment (PPE) and decentralized testing, the very facilities meant to contain the virus instead become engines of amplification.
“No one really has a full understanding of how serious this crisis is,” stated a Bunia-based U.N. official, reflecting the disconnect between the rapidly evolving biological threat and the stagnant resources on the ground.
4. A Perfect Storm: Conflict, Mining, and the Repatriation Factor
Containment efforts are currently being suffocated by a “perfect storm” of geography and social upheaval. The epicenter in Mongbwalu is a high-mobility mining zone located over 1,000 kilometers from the capital of Kinshasa, where road networks are poor and 273,000 people have already been displaced by armed conflict.
The “smoking gun” of this outbreak’s escalation was a logistical failure: the body of the first victim was repatriated from Bunia back to the Mongbwalu mining health zone for burial, inadvertently seeding the virus into a highly mobile population. This mobility has already carried the threat to major urban centers. In a chilling detail for contact tracers, a 59-year-old victim who later died in Kampala, Uganda, reportedly traveled from the DRC using public transportation, potentially exposing countless individuals along a major transit corridor. Meanwhile, fear-based measures like Rwanda’s border closure are proving counterproductive, pushing desperate travelers toward unmonitored informal crossings where they bypass all health screenings.
5. The Surveillance Gap: The Cost of Global Budget Cuts
This outbreak’s late detection was not an accident of biology; it was a predictable outcome of political and financial disinvestment. The dismantling of global health safety nets has left the world dangerously exposed.
The withdrawal of funding from the World Health Organization (WHO) during the Trump administration, combined with deep cuts to frontline USAID programs, dismantled the very surveillance infrastructure designed to catch rare variants before they reach urban centers. We are currently witnessing the bitter irony of global health policy: the funds “saved” by scaling back these programs are now being dwarfed by the massive economic and human cost of a response that started weeks too late.
Conclusion: Beyond the Border
The WHO has officially designated the Bundibugyo outbreak a “Public Health Emergency of International Concern” (PHEIC). While the agency notes that the situation does not yet meet the criteria for a pandemic, the window for containment is closing. As health teams scramble to establish treatment centers 1,000 kilometers from the central government’s reach, the world is forced to confront a sobering investigative truth.
Our global health security is only as strong as our ability to detect the unexpected. If our diagnostic tools and surveillance budgets are only calibrated for the “standard” threats we anticipate, we remain perpetually vulnerable to the pathogens that refuse to fit the mold. The question is no longer whether another rare variant will emerge, but whether we will have the courage to fund the systems required to see it coming.
Mystery at Sea: The Deadly Hantavirus Outbreak on an Expedition Cruise

A rare and terrifying medical emergency has been unfolding over the last few weeks on an expedition cruise ship. What started as an adventure to some of the world’s most remote locations quickly turned into a deadly crisis involving a little-known, yet incredibly dangerous, pathogen: the Hantavirus.
The Unfolding Crisis on the MV Hondius On April 1, 2026, the Dutch-flagged MV Hondius, operated by Oceanwide Expeditions, departed from Ushuaia, Argentina, with 147 passengers and crew on board. The vessel was scheduled to tour the ecologically diverse and remote regions of Antarctica and the South Atlantic islands.
Just days into the voyage on April 6, a 70-year-old Dutch passenger fell ill with a fever, headache, and mild diarrhea. His condition rapidly deteriorated into respiratory distress, and he tragically died on board on April 11. Over the following weeks, a terrifying cluster of severe respiratory illness emerged among the passengers. His 69-year-old wife, who had disembarked with his body at St. Helena, died shortly after arriving at an emergency department in South Africa. Another British passenger fell critically ill with pneumonia and had to be medically evacuated to an ICU in South Africa, while a fourth passenger, a German woman, died on the ship on May 2.
It took nearly a month from the first illness for laboratory officials in South Africa to finally confirm the culprit: Hantavirus. In total, the outbreak has resulted in three deaths, one critical hospitalization, and three other suspected cases remaining on the ship.
Currently, the ship is moored off the coast of Cape Verde waiting for emergency medical evacuations, while passengers remain under maximum physical distancing lockdowns in their cabins. Authorities suspect the initial exposure may have occurred when the first two victims traveled through Argentina before boarding, as the “Andes” strain of the hantavirus is endemic to South America.
Summary of cases from World Health Organization (WHO):
Case 1: An adult male developed symptoms of fever, headache, and mild diarrhoea on 6 April 2026 while on board the ship. By 11 April, the case developed respiratory distress and died on board on the same day. No microbiological tests were performed. The body of the passenger was removed from the vessel to Saint Helena (a British Overseas Territory) on 24 April.
Case 2: An adult female, who was a close contact of case 1, went ashore at Saint Helena on 24 April 2026 with gastrointestinal symptoms. She subsequently deteriorated during a flight to Johannesburg, South Africa, on 25 April. She later died upon arrival at the emergency department on 26 April. On 4 May, the case was subsequently confirmed by PCR with hantavirus infection. Contact tracing for passengers on the flight has been initiated.
Cases 1 and 2, had travelled in South America, including Argentina, before they boarded the cruise ship on 1 April 2026.
Case 3: An adult male presented to the ship’s doctor on 24 April 2026 with febrile illness, shortness of breath and signs of pneumonia. On 26 April, his condition worsened. He was medically evacuated from Ascension to South Africa on 27 April, where he is currently hospitalised in an Intensive Care Unit (ICU). Laboratory testing on an extensive respiratory pathogen panel was negative; however, polymerase chain reaction (PCR) testing confirmed hantavirus infection on 2 May 2026. Serology, sequencing and metagenomics are ongoing.
Case 4: An adult female, with presentation of pneumonia, died on 2 May 2026. The onset of symptoms was on 28 April, with fever and a general feeling of being unwell.Three suspected cases have reported high fever and/or gastrointestinal symptoms and remain on board. Medical teams in Cabo Verde are evaluating the patients and collecting additional specimens for testing.
What Exactly is Hantavirus? Hantaviruses are a family of viruses that are spread mainly by rodents. People typically contract the virus by coming into close contact with the urine, feces, or saliva of infected rodents, such as rats and mice. While rare, the virus can also be transmitted through rodent bites or scratches.
Generally, hantaviruses do not spread from person to person. However, there have been rare but documented instances of limited human-to-human transmission associated specifically with the Andes virus found in South America. However, there is a rare exception. In these uncommon instances, the virus can spread between people through close and prolonged contact in community settings. There have also been rare instances of secondary infections documented among healthcare workers in healthcare facilities.
Symptoms to Watch Out For Depending on the specific virus and region, hantaviruses typically cause two severe syndromes:
- Hantavirus Pulmonary Syndrome (HPS): Found mostly in the Western Hemisphere (including the U.S., Canada, and South America), this deadly disease severely affects the lungs. Early symptoms appear 1 to 8 weeks after exposure and look a lot like the flu—fatigue, fever, and severe muscle aches, particularly in the thighs, hips, and back. After 4 to 10 days, the late-stage symptoms set in, and patients develop coughing and shortness of breath as their lungs rapidly fill with fluid. HPS is extremely dangerous, with a fatality rate of up to 38% to 50% in the Americas.
- Hemorrhagic Fever with Renal Syndrome (HFRS): Found primarily in Europe and Asia, this syndrome severely impacts the kidneys. Symptoms appear within 1 to 2 weeks and include sudden intense headaches, back and abdominal pain, fever, nausea, and blurred vision. As the disease progresses, patients may experience low blood pressure, internal bleeding, acute shock, and acute kidney failure.
Treatment and Prevention Currently, there is no specific antiviral treatment, cure, or vaccine for hantavirus infections. Patients must rely on immediate supportive medical care in an intensive care unit. This care may involve intubation for breathing support in HPS cases, or dialysis to remove toxins from the blood in HFRS cases when the kidneys are failing. Antibiotics are also not routinely used unless a concurrent bacterial infection is suspected. While the antiviral drug ribavirin has shown some efficacy in treating Hemorrhagic Fever with Renal Syndrome (HFRS), it is not effective or licensed for treating the lung-affecting Hantavirus Pulmonary Syndrome.
Because there is no cure, treatment relies entirely on immediate supportive medical care, and early referral to an intensive care unit (ICU) is critical for improving a patient’s chances of survival. This supportive care may involve:
- Rest, hydration, and medications to manage fever and pain.
- Careful fluid administration and blood pressure (hemodynamic) monitoring.
- Respiratory support for patients experiencing breathing difficulties, which can include intubation, mechanical ventilation, or even extracorporeal mechanical oxygenation in severe cases.
- Dialysis for patients experiencing acute kidney failure to help remove toxins from the blood and balance fluids.
To protect yourself from hantavirus, health authorities recommend eliminating or minimizing contact with rodents in your home, workplace, or campsite. This includes sealing holes and gaps to keep rodents out, placing traps to decrease infestations, and immediately cleaning up any easily accessible food that might attract mice and rats. If you suspect you have been exposed to rodents and develop symptoms like fever, deep muscle aches, and severe fatigue, you should see a physician immediately and mention the potential exposure.

Zika Virus: Global Public Health Emergency


World Health Organization (WHO): Zika Virus is a Public Health Emergency of International Concern (PHEIC)
The first meeting of the Emergency Committee (EC) convened by the Director-General under the International Health Regulations (2005) (IHR 2005) regarding clusters of microcephaly cases and other neurologic disorders in some areas affected by Zika virus was held by teleconference on 1 February 2016, from 13:10 to 16:55 Central European Time.
The WHO Secretariat briefed the Committee on the clusters of microcephaly and Guillain-Barré Syndrome (GBS) that have been temporally associated with Zika virus transmission in some settings. The Committee was provided with additional data on the current understanding of the history of Zika virus, its spread, clinical presentation and epidemiology.
The following States Parties provided information on a potential association between microcephaly and/or neurological disorders and Zika virus disease: Brazil, France, United States of America, and El Salvador.
The Committee advised that the recent cluster of microcephaly cases and other neurologic disorders reported in Brazil, following a similar cluster in French Polynesia in 2014, constitutes a Public Health Emergency of International Concern (PHEIC).
Based on this information, the WHO Director-General declared a Public Health Emergency of International Concern (PHEIC) on 1 February 2016.
Aleppo Evil: The Skin Disfiguring Parasite Spreading across Syria
Sandflies & Civil War
The Syrian civil war has set the stage for the reemergence of a rare infectious disease. Transmitted through the bite of the sandfly, Leishmaniasis is a parasite that can affect many different parts of the body. The most prevalent form in the Middle East is called Cutaneous Leishmaniasis, which causes disfiguring welts and scarring of the skin. A more lethal variant known as Visceral Leishmaniasis can also damage the spleen and liver.
Since the Syrian conflict began in 2011, the number of Leishmaniasis cases has skyrocketed from 3,000 to over 100,000. Water shortages and poor sanitation have combined to create conditions ripe for the transmission of the disease. To make matters worse, the pentavalent antimonial drugs used to treat Leishmaniasis are becoming increasingly scarce. In times of conflict, Public Health tools such as surveillance, multi-sector response, and international collaboration rapidly diminish states Dr. Peter Hotez, Dean of the National School of Tropical Medicine at Baylor College of Medicine and President of the Sabin Vaccine Institute.

A Syrian refugee being treated for Leishmaniasis in Kilis, Turkey
Deadly Ebola Virus Ravaging Africa
Severe Pandemic in West Africa
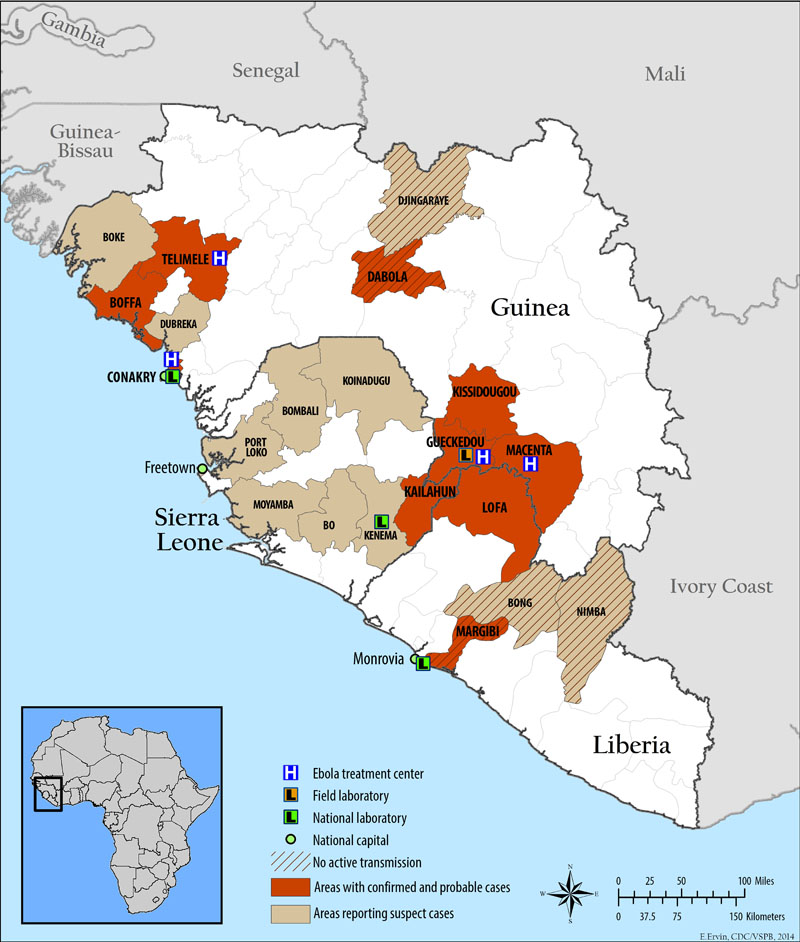
A deadly pandemic has been brewing in western Africa since December 2013. This latest outbreak of the deadly Ebola Virus Disease (EVD) began in the Republic of Guinea and then spread to Sierra Leone and Liberia. To date, 344 suspected and confirmed cases of EVD have been reported in Guinea, 112 in Sierra Leone, and 13 in Libera. Since emerging in 1976 in Sudan and Congo, EVD outbreaks have occurred 33 times.
Courtesy of the CDC
Spread of Ebola, Courtesy of Relief Web International
Syndromic Surveillance: Is Big Brother Looking Out for You?
On May 15, 2014, The New York Times reported about a program implemented in New Orleans which mined patient personal health information to identify which parents to warn prior to an impending ice storm. Dialysis patients were advised to get their treatments early, and those on ventilators were called so they knew how to get help if the power went out. New Orleans city officials knew whom to contact based on submitted Medicare claim requests. This data is now available for public emergency response and preparedness through the Federal Privacy Act of 1974.
Middle East Respiratory Syndrome (MERS): Global Travel Raises Concerns for Spread of Disease from the Arabian Peninsula
Middle East Respiratory Syndrome-Coronavirus (MERS-CoV), a novel Coronavirus in the same family as the Coronavirus that caused Severe Acute Respiratory Syndrome (SARS), has caused 339 illnesses and 102 deaths in Saudi Arabia . However, the WHO has only reported 262 laboratory-confirmed cases. Six Middle Eastern countries have reported MERS (Saudi Arabia, Qatar, United Arab Emirates, Jordan, Oman, Kuwait) and 5 other countries have reported traveler-associated MERS cases (United Kingdom, France, Tunisia, Italy, Malaysia). On May 2nd, the United States became the 6th county to report a traveler-associated MERS case. According to the CDC, an American healthcare worker flew back to the US from Saudi Arabia on April 24th, connecting in London and Chicago before taking a bus to Indiana. He is currently hospitalized and in stable condition. US Public Health officials are tracing the US MERS patient’s travel itinerary and attempting to contact other travelers who may have been in close contact with the affected individual. Currently, the US government has not issued any warnings to travelers to avoid the affected countries or to change travel plans.
