Syndromic Surveillance: Is Big Brother Looking Out for You?
On May 15, 2014, The New York Times reported about a program implemented in New Orleans which mined patient personal health information to identify which parents to warn prior to an impending ice storm. Dialysis patients were advised to get their treatments early, and those on ventilators were called so they knew how to get help if the power went out. New Orleans city officials knew whom to contact based on submitted Medicare claim requests. This data is now available for public emergency response and preparedness through the Federal Privacy Act of 1974.
Louisiana is not the only state implementing a program like this, with New York, Arizona, North Carolina, and others utilizing data collected through what is called Syndromic Surveillance.
Syndromic surveillance is the gathering of data for public health purposes before laboratory or clinically confirmed information is available. Interest in syndromic surveillance has increased because of concerns about bioterrorism. In addition to bioterrorism detection, syndromic surveillance may be suited to detecting waterborne disease outbreaks. Theoretical benefits of syndromic surveillance include potential timeliness, increased response capacity, ability to establish baseline disease burdens, and ability to delineate the geographical reach of an outbreak.
– Berger M, Shiau R, Winetraub J. Review of Syndromic Surveillance: Implications for Water-borne Disease Detection. J Epidemiol Community Health. Jun 2006; 60(6): 543–550.
Data which can be picked up through Syndromic Surveillance can be divided into two categories:
- Pre-Clinical: Data such as school and work absenteeism, calls to nurses or poison control centers, etc.
- Clinical Pre-Diagnostic: Listings of emergency department chief complaints, ambulance dispatch data or ICD codes
Syndromic surveillance, unlike traditional surveillance, focuses on pre-diagnostic data points rather than relying on official diagnoses, leading to more timely interventions to be implemented. This data, however, is much less specific than diagnostic data.
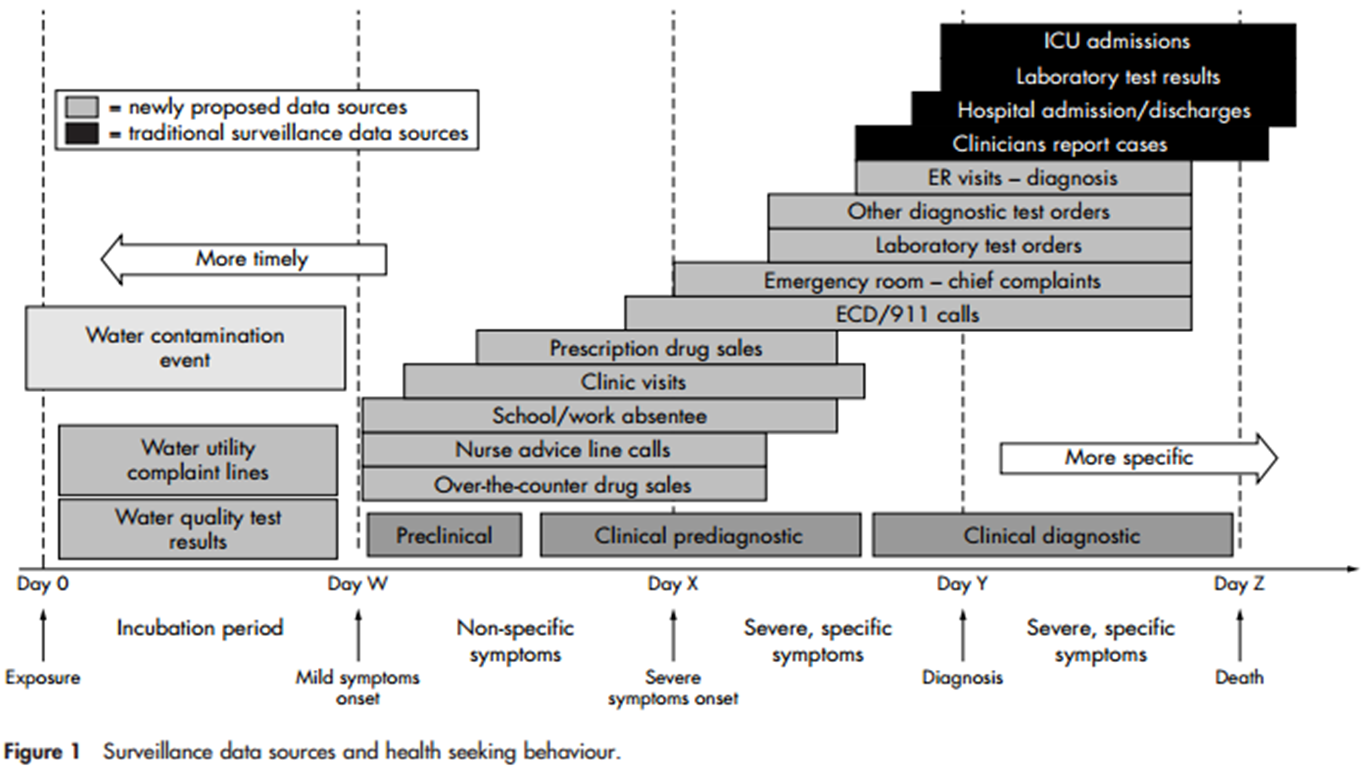
Surveillance data sources and health seeking behavior
Berger et. al performed a systematic review of studies done on Syndromic Surveillance and found that data collected was “best suited for detecting diseases that have a narrow incubation period distribution, a steep epidemic curve, a long prodromal phase, are not included on routine diagnostic tests, and do not have a specific disease identifying clinical feature.”
The use of syndromic surveillance has also been investigated for use in the event of a BioTerrorist emergency. A panel of experts were consulted in Duval County, FL to assess how the County could better utilize resources to prepare for and respond to such an event. This panel found that while there is potential for a great deal of information to be collected, it is imperative for cities to identify which resources and data sets to tap well before disaster strikes.
The CDC’s program for Syndromic Surveillance is called BioSense and utilizes data collected from the Department of Defense, the VA hospitals, and from private hospitals through LabCorp(R) test orders. Through BioSense, data can be shared across the country to track outbreaks that cross jurisdictional lines. This data has been utilized during the H1N1 Flu Pandemic of ’09-’10, the 2010 Deepwater Horizon Oil Spill, and in a 2012 Dengue Detection program in Florida and Hawaii among others. The BioSense program is run through the CDC’s Division of Health Informatics and Surveillance, which also runs the National Notifiable Diseases Surveillance System.
Of course, the thought of the government ‘data mining’ through personal health records is thought to be unnerving to some and measures to ensure HIPAA rules are necessary to prevent abuse. Are the potential benefits of Syndromic Surveillance worth the compromise in privacy?
—
For more examples of Syndromic Surveillance in action, review this article published in Morbidity and Mortality Weekly Report and the International Society for Disease Surveillance.
Report written by Vidya Eswaran
