Zika Virus: Global Public Health Emergency


World Health Organization (WHO): Zika Virus is a Public Health Emergency of International Concern (PHEIC)
The first meeting of the Emergency Committee (EC) convened by the Director-General under the International Health Regulations (2005) (IHR 2005) regarding clusters of microcephaly cases and other neurologic disorders in some areas affected by Zika virus was held by teleconference on 1 February 2016, from 13:10 to 16:55 Central European Time.
The WHO Secretariat briefed the Committee on the clusters of microcephaly and Guillain-Barré Syndrome (GBS) that have been temporally associated with Zika virus transmission in some settings. The Committee was provided with additional data on the current understanding of the history of Zika virus, its spread, clinical presentation and epidemiology.
The following States Parties provided information on a potential association between microcephaly and/or neurological disorders and Zika virus disease: Brazil, France, United States of America, and El Salvador.
The Committee advised that the recent cluster of microcephaly cases and other neurologic disorders reported in Brazil, following a similar cluster in French Polynesia in 2014, constitutes a Public Health Emergency of International Concern (PHEIC).
Based on this information, the WHO Director-General declared a Public Health Emergency of International Concern (PHEIC) on 1 February 2016.
Rapidly Emerging Threat
The Zika Virus was a scarcely known disease even in the final months of 2015. However, with the stunning epidemiological correlation that the Zika Virus may be linked to birth defects such as microcephaly (an abnormally small head) in children born to pregnant women infected with the disease, many countries in Latin American began raising warnings about the infection. Brazil was one of the first countries to recognize the concerning association between the Zika Virus infection and babies with rare brain birth defects. In October 2015, Dr. Vanessa Van Der Linden, a neurologist in the city of Recife, alerted state health officials about unusually high numbers of daily cases of microcephaly in babies of women who also reported mild viral symptoms and a rash during pregnancy. Dr. Van Der Linden determined the infections during pregnancy were too mild for more well known viral illnesses in the region such as dengue or chikungunya, and the link between Zika Virus and microcephaly began to emerge. In 2013 and 2014, Brazil had approximately 150 cases of microcephaly, and as of January 2016, Brazil reports more than 4,100 cases. Brazilian government officials suspect that the virus was introduced into the country during the 2014 Football (Soccer) World Cup games.
The virus was identified for the first time in 1947 in the Zika forest of Uganda in rhesus monkeys and then in 1952 in humans, and the virus has remained primarily in Africa except for sporadic outbreaks in Asia. In 2007, a major epidemic was reported on the island of Yap (Micronesia) when almost 75% of the population was infected.
The disease is spread via the bite of an infected Aedes aegypti mosquito, and nearly 80% of infected individuals have no symptoms. When patients do have symptoms, they begin 2-7 days after the bite of an infected mosquito and include:
- Mild fever
- Exanthema (skin rash)
- Conjunctivitis
- Muscle or joint pain
- General malaise
The symptoms last for a few days to a week. Individuals should contact their physicians if they develop symptoms within 2 weeks of traveling to a country with known Zika Virus transmission for possible testing and evaluation.
Treatment is supportive care and includes:
- Rest
- Plenty of fluids to avoid dehydration
- Pain control with acetaminophen (Tylenol)
- Avoid taking aspirin or other non-steroidal anti-inflammatory drugs (NSAIDs), like ibuprofen and naproxen
Current Health Security Risks
Active Zika Virus transmission is currently located in multiple countries in Central America, South America, and the Caribbean (see map). Women who are pregnant are strongly urged by the U.S. Centers for Disease Control (CDC) and the WHO to postpone travel to these regions.
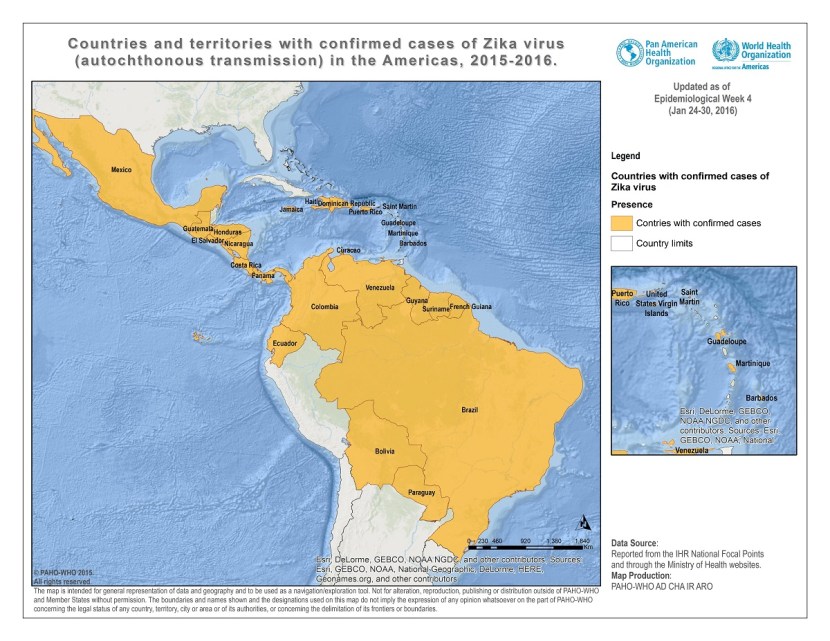
Courtesy of http://www.paho.org
Pregnancy and Zika Virus
The US CDC has provided physicians with the following protocol for evaluating pregnant women who have signs and symptoms of Zika Virus and have travelled to a country with active disease transmission within the past 2 weeks:

Courtesy of http://www.cdc.gov
WHO Emergency Committee Recommendations
The Committee provided the following advice to the Director-General to address the Zika Virus PHEIC:
Microcephaly and neurologic disorders
- Surveillance for microcephaly and GBS should be standardized and enhanced, particularly in areas of known Zika virus transmission and areas at risk of such transmission.
- Research into the etiology of new clusters of microcephaly and neurologic disorders should be intensified to determine whether there is a causative link to Zika virus and/or other factors or co-factors.
As these clusters have occurred in areas newly infected with Zika virus, and in keeping with good public health practice and the absence of another explanation for these clusters, the Committee highlights the importance of aggressive measures to reduce infection with Zika virus, particularly among pregnant women and women of childbearing age.
Zika virus transmission
- Surveillance for Zika virus infection should be enhanced, with the dissemination of standard case definitions and diagnostics to at-risk areas.
- The development of new diagnostics for Zika virus infection should be prioritized to facilitate surveillance and control measures.
- Risk communications should be enhanced in countries with Zika virus transmission to address population concerns, enhance community engagement, improve reporting, and ensure application of vector control and personal protective measures.
- Vector control measures and appropriate personal protective measures should be aggressively promoted and implemented to reduce the risk of exposure to Zika virus.
- Attention should be given to ensuring women of childbearing age and particularly pregnant women have the necessary information and materials to reduce risk of exposure.
- Pregnant women who have been exposed to Zika virus should be counselled and followed for birth outcomes based on the best available information and national practice and policies.
Longer-term measures
- Appropriate research and development efforts should be intensified for Zika virus vaccines, therapeutics and diagnostics.
- In areas of known Zika virus transmission health services should be prepared for potential increases in neurological syndromes and/or congenital malformations.
Travel measures
- There should be no restrictions on travel or trade with countries, areas and/or territories with Zika virus transmission.
- Travellers to areas with Zika virus transmission should be provided with up to date advice on potential risks and appropriate measures to reduce the possibility of exposure to mosquito bites.
- Standard WHO recommendations regarding disinsection of aircraft and airports should be implemented.
Data sharing
- National authorities should ensure the rapid and timely reporting and sharing of information of public health importance relevant to this PHEIC.
- Clinical, virologic and epidemiologic data related to the increased rates of microcephaly and/or GBS, and Zika virus transmission, should be rapidly shared with WHO to facilitate international understanding of the these events, to guide international support for control efforts, and to prioritize further research and product development.
