Category: Infectious Diseases Emergencies
Why a Rare Ebola Variant is Currently Outpacing Global Science: 5 Critical Takeaways
Introduction: The Ghost in the System
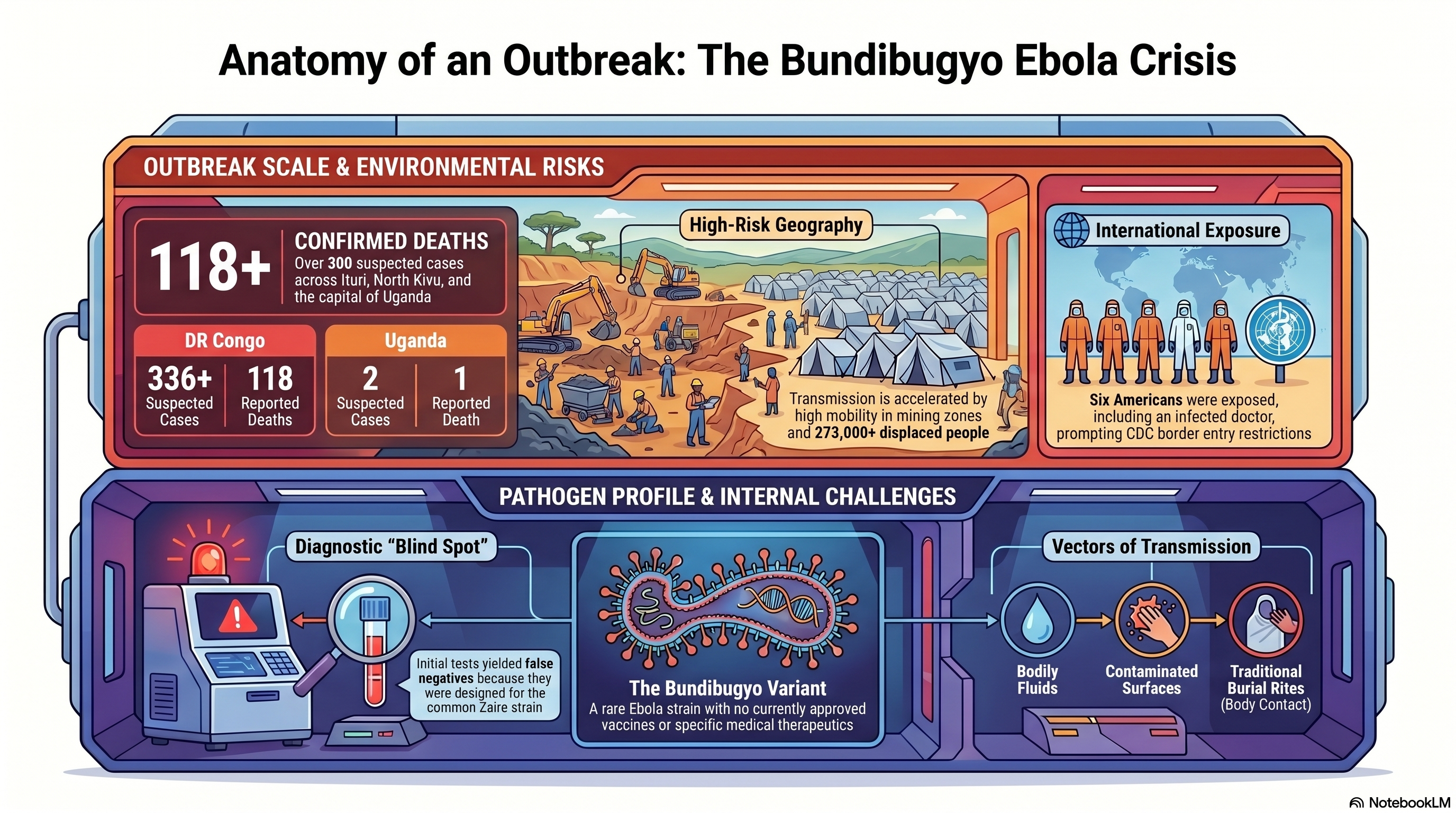
In the modern landscape of high-speed digital surveillance and automated biosensors, we have allowed ourselves to believe that a pathogen can no longer move in total silence. That illusion shattered in late April 2026. In the Ituri province of the Democratic Republic of Congo (DRC), a “mystery” illness began carving a path through remote mining communities, eventually escalating into a crisis that has now claimed 118 lives across the DRC and Uganda.
The culprit is the Bundibugyo Ebola virus—a rare, virulent strain that has appeared only three times since its discovery in 1976. This is not a simple resurgence of a familiar foe; it is a clinical and logistical outlier. While global health systems were calibrated for the common Zaire strain, Bundibugyo exploited our systemic blind spots, outpacing scientific intervention before the world even realized a race had begun.
1. The “Invisible” Strain: A Failure of Presumptive Testing
The Bundibugyo variant gained a lethal foothold because the global surveillance system is currently blind to its own gaps. When patients first presented with fever, muscle pain, and vomiting in late April, health officials deployed standard rapid field tests. These tests, however, were optimized for the Zaire strain. Because the symptoms mimicked other endemic tropical diseases, the negative results for Zaire Ebola provided a false sense of security that allowed the virus to circulate unhindered for weeks.
The diagnostic timeline reveals a catastrophic delay. It was not until May 14 that Ebola of any kind was confirmed, and only on May 15 was the Bundibugyo strain identified. By then, the virus had already infiltrated urban hubs like Bunia and crossed international borders.
“Because early tests looked for the wrong strain of Ebola, we got false negatives and lost weeks of response time,” says Matthew M. Kavanagh, director of the Georgetown University Center for Global Health Policy and Politics. “We are playing catch-up against a very dangerous pathogen.”
2. A Medical Blank Slate: The Zero-Vaccine Reality
The most harrowing reality for science communicators and health officials is the total absence of a medical safety net. Despite the massive research investment following the 2014-2016 West African epidemic, there are currently zero approved vaccines or therapeutics for the Bundibugyo strain.
Public health leaders are now forced into what Africa CDC Director General Dr. Jean Kaseya calls “panic mode.” While an experimental vaccine candidate exists, its data is a coin-flip: it has shown approximately 50% efficacy in primates, but its impact on humans is entirely unknown. For those on the ground, a 50% efficacy rate is a communication nightmare—it offers a glimmer of hope while simultaneously failing to provide the decisive protection needed to break the chain of transmission. This lack of tools is further complicated by cultural friction; Kaseya has issued urgent warnings regarding funeral practices, as traditional body-washing remains a primary driver of infection in the absence of pharmaceutical interventions.
3. The Frontline Vulnerability: High-Stakes Exposure
The surveillance gap has already exacted a heavy toll on the global and local medical community. In the provincial capital of Bunia, one American doctor has been laboratory-confirmed as an Ebola case. Furthermore, at least six other Americans have been exposed, prompting the U.S. CDC to coordinate their withdrawal and potential quarantine.
However, the deadliest impact remains local. In the Mongbwalu mining area, at least four healthcare workers died before the virus was even identified. This highlights the extreme risk of nosocomial (hospital-acquired) transmission. When clinics lack specialized Personal Protective Equipment (PPE) and decentralized testing, the very facilities meant to contain the virus instead become engines of amplification.
“No one really has a full understanding of how serious this crisis is,” stated a Bunia-based U.N. official, reflecting the disconnect between the rapidly evolving biological threat and the stagnant resources on the ground.
4. A Perfect Storm: Conflict, Mining, and the Repatriation Factor
Containment efforts are currently being suffocated by a “perfect storm” of geography and social upheaval. The epicenter in Mongbwalu is a high-mobility mining zone located over 1,000 kilometers from the capital of Kinshasa, where road networks are poor and 273,000 people have already been displaced by armed conflict.
The “smoking gun” of this outbreak’s escalation was a logistical failure: the body of the first victim was repatriated from Bunia back to the Mongbwalu mining health zone for burial, inadvertently seeding the virus into a highly mobile population. This mobility has already carried the threat to major urban centers. In a chilling detail for contact tracers, a 59-year-old victim who later died in Kampala, Uganda, reportedly traveled from the DRC using public transportation, potentially exposing countless individuals along a major transit corridor. Meanwhile, fear-based measures like Rwanda’s border closure are proving counterproductive, pushing desperate travelers toward unmonitored informal crossings where they bypass all health screenings.
5. The Surveillance Gap: The Cost of Global Budget Cuts
This outbreak’s late detection was not an accident of biology; it was a predictable outcome of political and financial disinvestment. The dismantling of global health safety nets has left the world dangerously exposed.
The withdrawal of funding from the World Health Organization (WHO) during the Trump administration, combined with deep cuts to frontline USAID programs, dismantled the very surveillance infrastructure designed to catch rare variants before they reach urban centers. We are currently witnessing the bitter irony of global health policy: the funds “saved” by scaling back these programs are now being dwarfed by the massive economic and human cost of a response that started weeks too late.
Conclusion: Beyond the Border
The WHO has officially designated the Bundibugyo outbreak a “Public Health Emergency of International Concern” (PHEIC). While the agency notes that the situation does not yet meet the criteria for a pandemic, the window for containment is closing. As health teams scramble to establish treatment centers 1,000 kilometers from the central government’s reach, the world is forced to confront a sobering investigative truth.
Our global health security is only as strong as our ability to detect the unexpected. If our diagnostic tools and surveillance budgets are only calibrated for the “standard” threats we anticipate, we remain perpetually vulnerable to the pathogens that refuse to fit the mold. The question is no longer whether another rare variant will emerge, but whether we will have the courage to fund the systems required to see it coming.
Mystery at Sea: The Deadly Hantavirus Outbreak on an Expedition Cruise

A rare and terrifying medical emergency has been unfolding over the last few weeks on an expedition cruise ship. What started as an adventure to some of the world’s most remote locations quickly turned into a deadly crisis involving a little-known, yet incredibly dangerous, pathogen: the Hantavirus.
The Unfolding Crisis on the MV Hondius On April 1, 2026, the Dutch-flagged MV Hondius, operated by Oceanwide Expeditions, departed from Ushuaia, Argentina, with 147 passengers and crew on board. The vessel was scheduled to tour the ecologically diverse and remote regions of Antarctica and the South Atlantic islands.
Just days into the voyage on April 6, a 70-year-old Dutch passenger fell ill with a fever, headache, and mild diarrhea. His condition rapidly deteriorated into respiratory distress, and he tragically died on board on April 11. Over the following weeks, a terrifying cluster of severe respiratory illness emerged among the passengers. His 69-year-old wife, who had disembarked with his body at St. Helena, died shortly after arriving at an emergency department in South Africa. Another British passenger fell critically ill with pneumonia and had to be medically evacuated to an ICU in South Africa, while a fourth passenger, a German woman, died on the ship on May 2.
It took nearly a month from the first illness for laboratory officials in South Africa to finally confirm the culprit: Hantavirus. In total, the outbreak has resulted in three deaths, one critical hospitalization, and three other suspected cases remaining on the ship.
Currently, the ship is moored off the coast of Cape Verde waiting for emergency medical evacuations, while passengers remain under maximum physical distancing lockdowns in their cabins. Authorities suspect the initial exposure may have occurred when the first two victims traveled through Argentina before boarding, as the “Andes” strain of the hantavirus is endemic to South America.
Summary of cases from World Health Organization (WHO):
Case 1: An adult male developed symptoms of fever, headache, and mild diarrhoea on 6 April 2026 while on board the ship. By 11 April, the case developed respiratory distress and died on board on the same day. No microbiological tests were performed. The body of the passenger was removed from the vessel to Saint Helena (a British Overseas Territory) on 24 April.
Case 2: An adult female, who was a close contact of case 1, went ashore at Saint Helena on 24 April 2026 with gastrointestinal symptoms. She subsequently deteriorated during a flight to Johannesburg, South Africa, on 25 April. She later died upon arrival at the emergency department on 26 April. On 4 May, the case was subsequently confirmed by PCR with hantavirus infection. Contact tracing for passengers on the flight has been initiated.
Cases 1 and 2, had travelled in South America, including Argentina, before they boarded the cruise ship on 1 April 2026.
Case 3: An adult male presented to the ship’s doctor on 24 April 2026 with febrile illness, shortness of breath and signs of pneumonia. On 26 April, his condition worsened. He was medically evacuated from Ascension to South Africa on 27 April, where he is currently hospitalised in an Intensive Care Unit (ICU). Laboratory testing on an extensive respiratory pathogen panel was negative; however, polymerase chain reaction (PCR) testing confirmed hantavirus infection on 2 May 2026. Serology, sequencing and metagenomics are ongoing.
Case 4: An adult female, with presentation of pneumonia, died on 2 May 2026. The onset of symptoms was on 28 April, with fever and a general feeling of being unwell.Three suspected cases have reported high fever and/or gastrointestinal symptoms and remain on board. Medical teams in Cabo Verde are evaluating the patients and collecting additional specimens for testing.
What Exactly is Hantavirus? Hantaviruses are a family of viruses that are spread mainly by rodents. People typically contract the virus by coming into close contact with the urine, feces, or saliva of infected rodents, such as rats and mice. While rare, the virus can also be transmitted through rodent bites or scratches.
Generally, hantaviruses do not spread from person to person. However, there have been rare but documented instances of limited human-to-human transmission associated specifically with the Andes virus found in South America. However, there is a rare exception. In these uncommon instances, the virus can spread between people through close and prolonged contact in community settings. There have also been rare instances of secondary infections documented among healthcare workers in healthcare facilities.
Symptoms to Watch Out For Depending on the specific virus and region, hantaviruses typically cause two severe syndromes:
- Hantavirus Pulmonary Syndrome (HPS): Found mostly in the Western Hemisphere (including the U.S., Canada, and South America), this deadly disease severely affects the lungs. Early symptoms appear 1 to 8 weeks after exposure and look a lot like the flu—fatigue, fever, and severe muscle aches, particularly in the thighs, hips, and back. After 4 to 10 days, the late-stage symptoms set in, and patients develop coughing and shortness of breath as their lungs rapidly fill with fluid. HPS is extremely dangerous, with a fatality rate of up to 38% to 50% in the Americas.
- Hemorrhagic Fever with Renal Syndrome (HFRS): Found primarily in Europe and Asia, this syndrome severely impacts the kidneys. Symptoms appear within 1 to 2 weeks and include sudden intense headaches, back and abdominal pain, fever, nausea, and blurred vision. As the disease progresses, patients may experience low blood pressure, internal bleeding, acute shock, and acute kidney failure.
Treatment and Prevention Currently, there is no specific antiviral treatment, cure, or vaccine for hantavirus infections. Patients must rely on immediate supportive medical care in an intensive care unit. This care may involve intubation for breathing support in HPS cases, or dialysis to remove toxins from the blood in HFRS cases when the kidneys are failing. Antibiotics are also not routinely used unless a concurrent bacterial infection is suspected. While the antiviral drug ribavirin has shown some efficacy in treating Hemorrhagic Fever with Renal Syndrome (HFRS), it is not effective or licensed for treating the lung-affecting Hantavirus Pulmonary Syndrome.
Because there is no cure, treatment relies entirely on immediate supportive medical care, and early referral to an intensive care unit (ICU) is critical for improving a patient’s chances of survival. This supportive care may involve:
- Rest, hydration, and medications to manage fever and pain.
- Careful fluid administration and blood pressure (hemodynamic) monitoring.
- Respiratory support for patients experiencing breathing difficulties, which can include intubation, mechanical ventilation, or even extracorporeal mechanical oxygenation in severe cases.
- Dialysis for patients experiencing acute kidney failure to help remove toxins from the blood and balance fluids.
To protect yourself from hantavirus, health authorities recommend eliminating or minimizing contact with rodents in your home, workplace, or campsite. This includes sealing holes and gaps to keep rodents out, placing traps to decrease infestations, and immediately cleaning up any easily accessible food that might attract mice and rats. If you suspect you have been exposed to rodents and develop symptoms like fever, deep muscle aches, and severe fatigue, you should see a physician immediately and mention the potential exposure.

Zika Virus: Global Public Health Emergency


World Health Organization (WHO): Zika Virus is a Public Health Emergency of International Concern (PHEIC)
The first meeting of the Emergency Committee (EC) convened by the Director-General under the International Health Regulations (2005) (IHR 2005) regarding clusters of microcephaly cases and other neurologic disorders in some areas affected by Zika virus was held by teleconference on 1 February 2016, from 13:10 to 16:55 Central European Time.
The WHO Secretariat briefed the Committee on the clusters of microcephaly and Guillain-Barré Syndrome (GBS) that have been temporally associated with Zika virus transmission in some settings. The Committee was provided with additional data on the current understanding of the history of Zika virus, its spread, clinical presentation and epidemiology.
The following States Parties provided information on a potential association between microcephaly and/or neurological disorders and Zika virus disease: Brazil, France, United States of America, and El Salvador.
The Committee advised that the recent cluster of microcephaly cases and other neurologic disorders reported in Brazil, following a similar cluster in French Polynesia in 2014, constitutes a Public Health Emergency of International Concern (PHEIC).
Based on this information, the WHO Director-General declared a Public Health Emergency of International Concern (PHEIC) on 1 February 2016.
Measles: Centuries Old Disease Causing 21st Century Public Health Crisis

(Courtesy cdc.gov)
Resurgence of a disease that was “eliminated” from the United States in 2000
In medical history, measles was 1st identified as a unique disease by the Persian physician Rhazes in the 9th century when he published the text titled The Book of Smallpox and Measles. Measles is an ancient disease that used to have a profound global impact causing hundreds of thousands of deaths and millions of cases each year. In the 16th century, a measles epidemic caused the deaths of two-thirds of the population of Cuba in one year, and two years later, it killed half the population of Honduras. In the 1850’s, a measles outbreak caused the death of 20% of the population of Hawaii. From 1840-1990, it is estimated that measles has killed approximately 200 million people worldwide.
International Health Regulations: WHO Framework to Combat Epidemics

WHO International Working Group on the Revision of the International Health Regulations (WHO/Jean-Marc Ferré)
Global Need for Coordination of Efforts
The International Health Regulations (IHR) is a structural body created to increase Global Health Security and prevent national public health emergencies from becoming global crises. The IHR were first implemented in 1969 focusing on plague, cholera, yellow fever and small pox. Several years later in 1995, the reemergence of plague in India and Ebola in Democratic Republic of Congo (DRC) created the need to revise and update the IHR. This led to the creation of a network of technical collaborations among existing institutions and networks, which would pool human and technical resources for the rapid identification, confirmation and response to outbreaks of international importance: the Global Outbreak Alert and Response Network (GOARN). Most recently, the GOARN has focused on the Middle East Respiratory Syndrome Coronavirus (MERS-CoV). Alert and response operations functions include:
- Event-based surveillance, multi-hazard rapid risk assessment and event-based risk communications
- Critical information and communications platforms for decision support
- Operations and logistics platforms for any WHO response to international public health risks.
Influenza 2014: Are We Prepared?

- (courtesy http://www.idsociety.org)
The flu season is just beginning
In the United States, the flu season typically spans from December to February. About 25,000 people die each year in the US from flu-related complications. The latest statistics from 2011 indicate 53,826 people died from influenza and pneumonia. The US Centers for Disease Control and Prevention (CDC) has designated December 7-13th as National Influenza Week to emphasize the public health need for flu vaccinations as we enter the peak flu season. Availability of the flu vaccine should be widely accessible, and 7 influenza vaccine manufacturers are projecting around 155 million doses of influenza vaccine will be available this year. The 2014-2015 influenza vaccine will protect against at least 3 strains of flu (trivalent vaccine), and an additional vaccine will be available that will also protect against a 4th strain (quadrivalent vaccine). All of the 2014-2015 influenza vaccines will protect against the following 3 strains:
- A/California/7/2009 (H1N1) pdm09-like virus
- A/Texas/50/2012 (H3N2)-like virus
- B/Massachusetts/2/2012-like virus
The quadrivalent vaccine will also add protection against additional B virus: B/Brisbane/60/2008-like virus.
Quarantine: Ethical & Legal Battle for Human Rights during Public Health Emergencies
As the Ebola Epidemic of 2014 continues, some officials are calling upon a centuries-old tactic to combat the disease: medical quarantine. In an effort that began on October 24th, New York and New Jersey state officials instituted a mandatory 21-day quarantine on all medical personnel returning from volunteer efforts to combat the disease in West Africa.

No Standard Protocols
While some states are embracing the idea and implementing quarantines of their own, other state and national officials are denouncing them. Medecins Sans Frontieres (MSF), the main humanitarian group coordinating volunteer efforts in Africa also denounced the quarantines:
There are other ways to adequately address both public anxiety and health imperatives, and the response to Ebola must not be guided primarily by panic in countries not overly affected by the epidemic,” said Sophie Delaunay, executive director of MSF-USA. “Any regulation not based on scientific medical grounds, which would isolate healthy aid workers, will very likely serve as a disincentive to others to combat the epidemic at its source, in West Africa.
International MSF staff members commit to burdensome four-to-six week assignments in the Ebola affected countries. The risk of being quarantined for 21 days upon completion of their work has already prompted some people to reduce their length of time in the field. Others will be less inclined to volunteer in the first place. This will present significant operational disruptions at the field level for MSF and other organizations, and lead to an overall shortage of desperately needed health workers, precisely when the Ebola outbreak is as out of control as ever.
Baylor College of Medicine Team Provides Ebola Training in Nigeria

City of Lagos (courtesy of nigeriaembassyusa.org)
In mid-September, a six-member team from Baylor College of Medicine trained nearly 1,500 healthcare providers and non-medical personnel in the basic facts about Ebola and in the care of people with the disease during four days of training in two Nigerian cities – Lagos, Africa’s most populous city, and Eket, an industrial city in the south. The effort was sponsored by ExxonMobil, which has offices and petroleum operations in the African nation.
Nigeria has had a limited number of cases of the disease in the current outbreak, and the disease has been designated as contained as of early October.
The Baylor training consisted of a presentation for the non-medical public about the disease itself and how best to protect against it. A second, more sophisticated presentation was designed for healthcare providers, describing the best methods to prevent transmission, caring for patients, and protecting against acquiring the infection during care. A third presentation dealt with the appropriate personal protective equipment and how best to put it on and take it off safely.
Dr. Bobby Kapur, physician leader and associate professor of medicine – emergency medicine at Baylor, said it was interesting that Nigeria’s situation was similar to that in the United States. One person traveled from Liberia to Nigeria and then had some contact within the community.
Enterovirus D68: Sweeping across the US
The respiratory virus known as Enterovirus D68 (EVD68) has been sweeping the country this summer, primarily infecting children. So far 691 people in 46 states have been infected. Luckily, enterovirus is typically a summer virus, and it’s season shall soon come to an end.
Children with Asthma may have Worse Outcomes with EVD68
While the signs and symptoms of EVD68 generally mirror that of other respiratory viruses and can include fever, runny nose, sneezing, cough, and body and muscle aches. In some children wheezing and difficulty breathing can develop. The most deadly form of the virus seems to be more widespread in the Midwest. At the peak of the Kansas City-area outbreak their 354-bed hospital was filled, and Children’s Mercy had 100 patients in their pediatric intensive care unit (PICU), three times more than normal for this time of year. Patients usually end up in the PICU due to severe bronchospasms, and often many children affected by the virus suffer from asthma or have had episodes of wheezing in the past. This video describes EVD68 in more depth.
Ebola: Hot Zone arrives in the Lone Star State
The 1st ever documented case of Ebola in the United States was announced on September 30, 2014 by the Centers for Disease Control & Prevention (CDC) and the Texas Department of State Health Services.

Ebola virus (Image courtesy dailytech.com)
Dallas, We have an Infection
Thomas Eric Duncan, a 42 year old Liberian national, who was traveling to the US for the 1st time to visit family in Dallas arrived in Texas on September 20, 2014. He had traveled to Dallas via flights from Brussels to Washington, DC then to Dallas. Mr. Duncan, initially showed signs of a low-grade fever and abdominal pain beginning on September 24th and was seen at Texas Health Presbyterian Hospital Dallas on September 26th. Although his family had informed the healthcare workers of his recent arrival from Liberia, the hospital personnel decided he did not meet the criteria for Ebola suspicion since he did not have a temperature greater than 101.5 degrees Fahrenheit. He was discharged home. On September 28th, Mr. Duncan’s symptoms worsened, and he was transported by Dallas County EMS back to Presbyterian Hospital and was placed into isolation. On September 30th, lab tests from the State of Texas and the CDC confirmed the patient has Ebola. He is currently in critical condition in the ICU. The C.D.C. has sent a team to Dallas to identify others who may have contracted the illness.

Texas Health Presbyterian Hospital. (courtesy of NPR.com)
It is important to remember that Ebola does not have respiratory transmission. The disease is only spread through exchange of bodily fluids and is only contagious when symptoms appear. Thus, only those who interacted with Mr. Duncan on or after September 24th are at risk. The Director of the CDC, Dr. Thomas Frieden has stated there is “zero risk of transmission” to fellow passengers on his flights because he was not showing signs of symptoms while traveling.
