Tagged: travel
Why a Rare Ebola Variant is Currently Outpacing Global Science: 5 Critical Takeaways
Introduction: The Ghost in the System
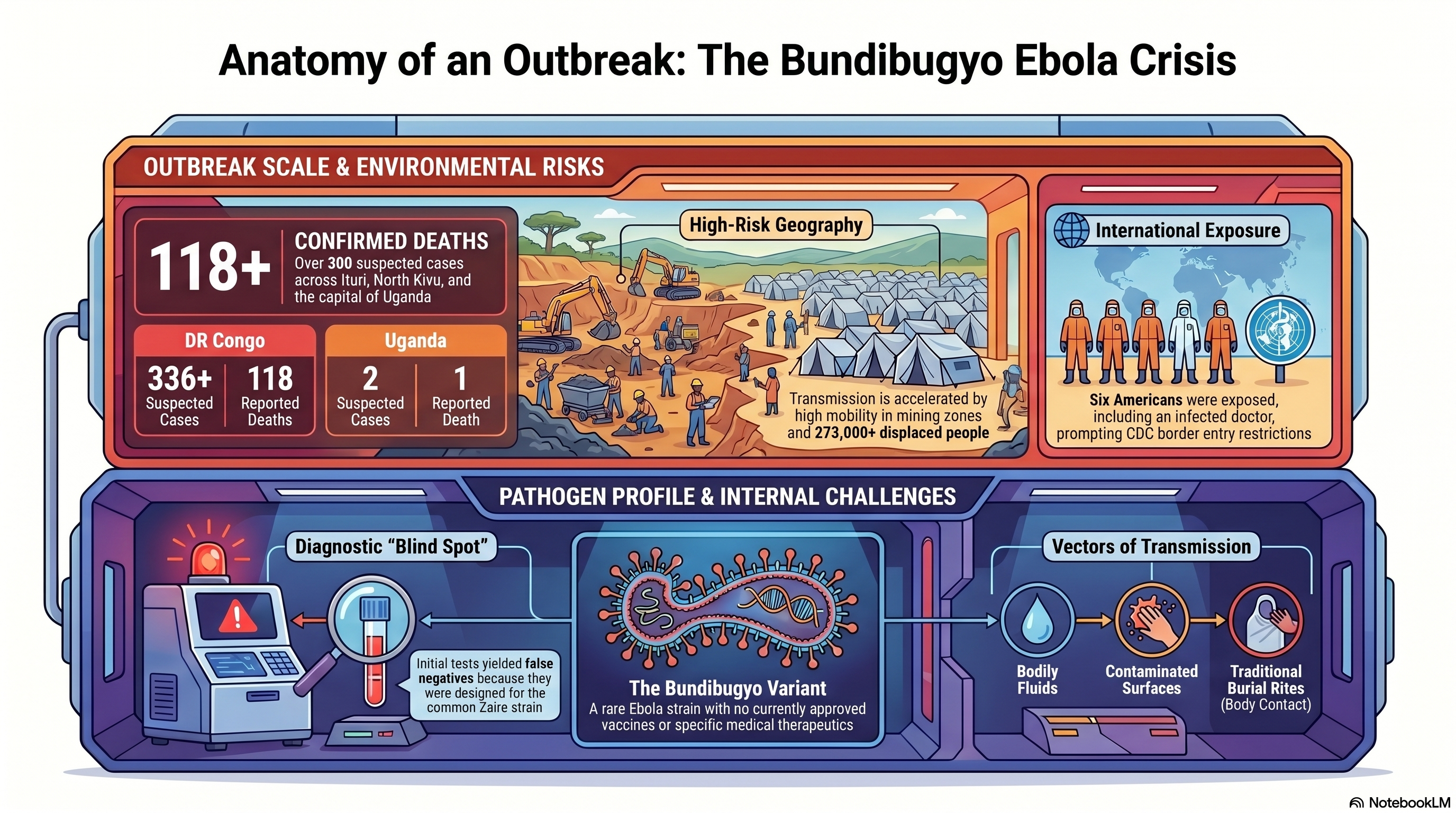
In the modern landscape of high-speed digital surveillance and automated biosensors, we have allowed ourselves to believe that a pathogen can no longer move in total silence. That illusion shattered in late April 2026. In the Ituri province of the Democratic Republic of Congo (DRC), a “mystery” illness began carving a path through remote mining communities, eventually escalating into a crisis that has now claimed 118 lives across the DRC and Uganda.
The culprit is the Bundibugyo Ebola virus—a rare, virulent strain that has appeared only three times since its discovery in 1976. This is not a simple resurgence of a familiar foe; it is a clinical and logistical outlier. While global health systems were calibrated for the common Zaire strain, Bundibugyo exploited our systemic blind spots, outpacing scientific intervention before the world even realized a race had begun.
1. The “Invisible” Strain: A Failure of Presumptive Testing
The Bundibugyo variant gained a lethal foothold because the global surveillance system is currently blind to its own gaps. When patients first presented with fever, muscle pain, and vomiting in late April, health officials deployed standard rapid field tests. These tests, however, were optimized for the Zaire strain. Because the symptoms mimicked other endemic tropical diseases, the negative results for Zaire Ebola provided a false sense of security that allowed the virus to circulate unhindered for weeks.
The diagnostic timeline reveals a catastrophic delay. It was not until May 14 that Ebola of any kind was confirmed, and only on May 15 was the Bundibugyo strain identified. By then, the virus had already infiltrated urban hubs like Bunia and crossed international borders.
“Because early tests looked for the wrong strain of Ebola, we got false negatives and lost weeks of response time,” says Matthew M. Kavanagh, director of the Georgetown University Center for Global Health Policy and Politics. “We are playing catch-up against a very dangerous pathogen.”
2. A Medical Blank Slate: The Zero-Vaccine Reality
The most harrowing reality for science communicators and health officials is the total absence of a medical safety net. Despite the massive research investment following the 2014-2016 West African epidemic, there are currently zero approved vaccines or therapeutics for the Bundibugyo strain.
Public health leaders are now forced into what Africa CDC Director General Dr. Jean Kaseya calls “panic mode.” While an experimental vaccine candidate exists, its data is a coin-flip: it has shown approximately 50% efficacy in primates, but its impact on humans is entirely unknown. For those on the ground, a 50% efficacy rate is a communication nightmare—it offers a glimmer of hope while simultaneously failing to provide the decisive protection needed to break the chain of transmission. This lack of tools is further complicated by cultural friction; Kaseya has issued urgent warnings regarding funeral practices, as traditional body-washing remains a primary driver of infection in the absence of pharmaceutical interventions.
3. The Frontline Vulnerability: High-Stakes Exposure
The surveillance gap has already exacted a heavy toll on the global and local medical community. In the provincial capital of Bunia, one American doctor has been laboratory-confirmed as an Ebola case. Furthermore, at least six other Americans have been exposed, prompting the U.S. CDC to coordinate their withdrawal and potential quarantine.
However, the deadliest impact remains local. In the Mongbwalu mining area, at least four healthcare workers died before the virus was even identified. This highlights the extreme risk of nosocomial (hospital-acquired) transmission. When clinics lack specialized Personal Protective Equipment (PPE) and decentralized testing, the very facilities meant to contain the virus instead become engines of amplification.
“No one really has a full understanding of how serious this crisis is,” stated a Bunia-based U.N. official, reflecting the disconnect between the rapidly evolving biological threat and the stagnant resources on the ground.
4. A Perfect Storm: Conflict, Mining, and the Repatriation Factor
Containment efforts are currently being suffocated by a “perfect storm” of geography and social upheaval. The epicenter in Mongbwalu is a high-mobility mining zone located over 1,000 kilometers from the capital of Kinshasa, where road networks are poor and 273,000 people have already been displaced by armed conflict.
The “smoking gun” of this outbreak’s escalation was a logistical failure: the body of the first victim was repatriated from Bunia back to the Mongbwalu mining health zone for burial, inadvertently seeding the virus into a highly mobile population. This mobility has already carried the threat to major urban centers. In a chilling detail for contact tracers, a 59-year-old victim who later died in Kampala, Uganda, reportedly traveled from the DRC using public transportation, potentially exposing countless individuals along a major transit corridor. Meanwhile, fear-based measures like Rwanda’s border closure are proving counterproductive, pushing desperate travelers toward unmonitored informal crossings where they bypass all health screenings.
5. The Surveillance Gap: The Cost of Global Budget Cuts
This outbreak’s late detection was not an accident of biology; it was a predictable outcome of political and financial disinvestment. The dismantling of global health safety nets has left the world dangerously exposed.
The withdrawal of funding from the World Health Organization (WHO) during the Trump administration, combined with deep cuts to frontline USAID programs, dismantled the very surveillance infrastructure designed to catch rare variants before they reach urban centers. We are currently witnessing the bitter irony of global health policy: the funds “saved” by scaling back these programs are now being dwarfed by the massive economic and human cost of a response that started weeks too late.
Conclusion: Beyond the Border
The WHO has officially designated the Bundibugyo outbreak a “Public Health Emergency of International Concern” (PHEIC). While the agency notes that the situation does not yet meet the criteria for a pandemic, the window for containment is closing. As health teams scramble to establish treatment centers 1,000 kilometers from the central government’s reach, the world is forced to confront a sobering investigative truth.
Our global health security is only as strong as our ability to detect the unexpected. If our diagnostic tools and surveillance budgets are only calibrated for the “standard” threats we anticipate, we remain perpetually vulnerable to the pathogens that refuse to fit the mold. The question is no longer whether another rare variant will emerge, but whether we will have the courage to fund the systems required to see it coming.
