The 1st ever documented case of Ebola in the United States was announced on September 30, 2014 by the Centers for Disease Control & Prevention (CDC) and the Texas Department of State Health Services.
Ebola virus (Image courtesy dailytech.com)
Dallas, We have an Infection
Thomas Eric Duncan, a 42 year old Liberian national, who was traveling to the US for the 1st time to visit family in Dallas arrived in Texas on September 20, 2014. He had traveled to Dallas via flights from Brussels to Washington, DC then to Dallas. Mr. Duncan, initially showed signs of a low-grade fever and abdominal pain beginning on September 24th and was seen at Texas Health Presbyterian Hospital Dallas on September 26th. Although his family had informed the healthcare workers of his recent arrival from Liberia, the hospital personnel decided he did not meet the criteria for Ebola suspicion since he did not have a temperature greater than 101.5 degrees Fahrenheit. He was discharged home. On September 28th, Mr. Duncan’s symptoms worsened, and he was transported by Dallas County EMS back to Presbyterian Hospital and was placed into isolation. On September 30th, lab tests from the State of Texas and the CDC confirmed the patient has Ebola. He is currently in critical condition in the ICU. The C.D.C. has sent a team to Dallas to identify others who may have contracted the illness.
Texas Health Presbyterian Hospital. (courtesy of NPR.com)
It is important to remember that Ebola does not have respiratory transmission. The disease is only spread through exchange of bodily fluids and is only contagious when symptoms appear. Thus, only those who interacted with Mr. Duncan on or after September 24th are at risk. The Director of the CDC, Dr. Thomas Frieden has stated there is “zero risk of transmission” to fellow passengers on his flights because he was not showing signs of symptoms while traveling.
The authors of the accompanying article note that EVD is not the most transmissible virus – Measles currently holds that title. In fact, it is hypothesized that healthcare workers only need to stop 50% of infectious contacts via effective isolation to stem the epidemic. While isolation techniques have been hard to put into place in West Africa, it should be easy to do here in the United States. Therefore, there is very little risk of seeing an epidemic on a scale such that as that in Africa here in the US. The video below describes how the CDC uses Contact Tracing to try to stem outbreaks such as EVD.
Community-Based Surveillance
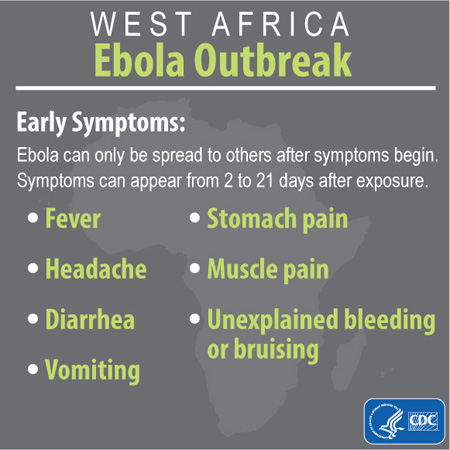
Remember, here is what you should be looking out for in patients who report recent contact with EVD patients or recent travel from West Africa:
Signs & Symptoms of EVD. Image courtesy of the CDC
While symptoms can appear anywhere from 2-21 days after exposure, the average is 8-10 days. Those who recover from EVD will retain antibodies to the disease for at least 10 years.
A fever of greater than 38.6 degrees Celsius or 101.5 degrees Fahrenheit
Additional symptoms such as severe headache, muscle pain, vomiting, diarrhea, abdominal pain, or unexplained hemorrhage;AND
Risk factors within the past 3 weeks before the onset of symptoms, such as contact with blood or other body fluids of a patient known to have or suspected to have EVD; residence in—or travel to—an area where EVD transmission is active; or direct handling of bats or nonhuman primates from disease-endemic areas. Malaria diagnostics should also be a part of initial testing because it is the most common cause of febrile illness in persons with a travel history to the affected countries.
If you suspect a patient has EVD, the following diagnostic tests are available:
Within a few days of appearance of symptoms:
Antigen-capture ELISA testing
IgM ELISA
EVD PCR
Virus Isolation
Later in disease course or after recovery:
IgM and IgG antibodies
In deceased patients:
Immunohistochemistry
PCR
Virus Isolation
The CDC recommends an individual be tested if the following are true:
percutaneous or mucous membrane exposure or direct skin contact with body fluids of a person with a confirmed or suspected case of EVD without appropriate personal protective equipment (PPE),
laboratory processing of body fluids of suspected or confirmed EVD cases without appropriate PPE or standard biosafety precautions, or
participation in funeral rites or other direct exposure to human remains in the geographic area where the outbreak is occurring without appropriate PPE.
For persons with a high-risk exposure but without a fever, testing is recommended only if there are other compatible clinical symptoms present and blood work findings are abnormal (i.e., thrombocytopenia <150,000 cells/µL and/or elevated transaminases).
If you have any suspicion of EVD, contact the CDC! The infographic below details exactly how to collect samples for testing.
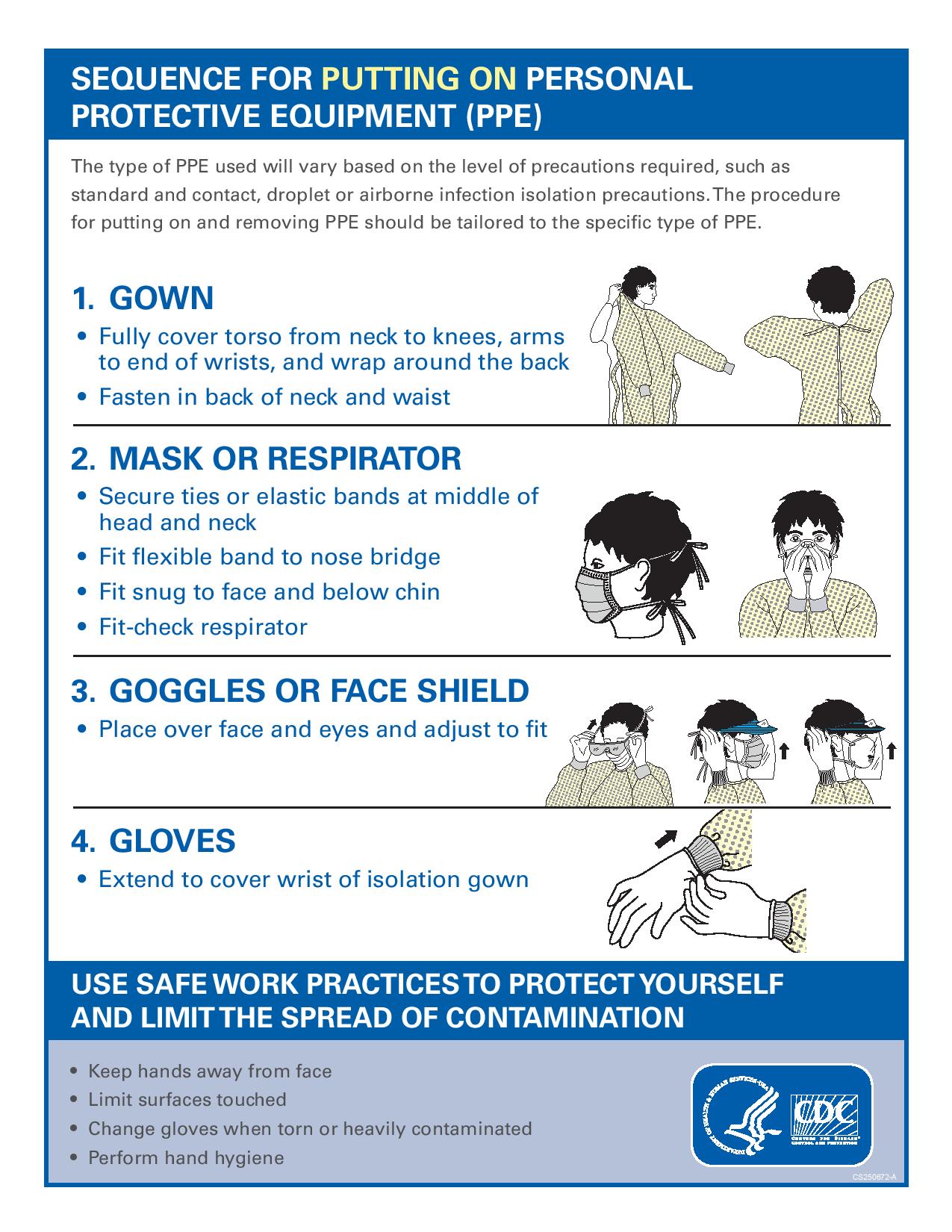
Healthcare Providers: Protect Thyself
In order to protect yourself and your fellow healthcare providers, proper PPE protection from all bodily fluids is crucial. This includes blood, emesis, sweat, feces, semen, etc. Use the guide below to ensure you are protected.
Single patient room (containing a private bathroom) with the door closed
Facilities should maintain a log of all persons entering the patient’s room
Consider posting personnel at the patient’s door to ensure appropriate and consistent use of PPE by all persons entering the patient room
Personal Protective Equipment (PPE)
All persons entering the patient room should wear at least:
Gloves
Gown (fluid resistant or impermeable)
Eye protection (goggles or face shield)
Facemask
Additional PPE might be required in certain situations (e.g., copious amounts of blood, other body fluids, vomit, or feces present in the environment), including but not limited to:
Double gloving
Disposable shoe covers
Leg coverings
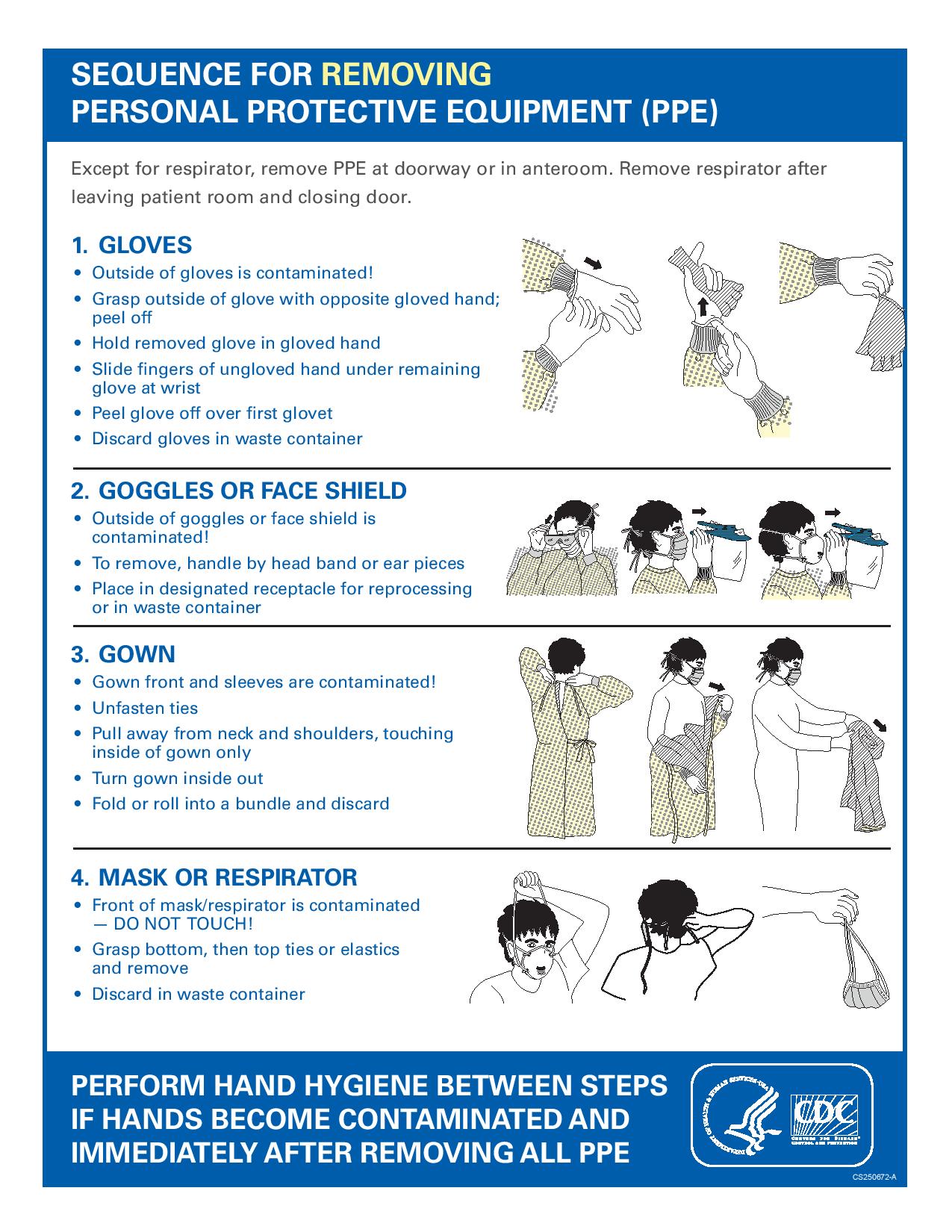
Recommended PPE should be worn by HCP upon entry into patient rooms or care areas. Upon exit from the patient room or care area, PPE should be carefully removed without contaminating one’s eyes, mucous membranes, or clothing with potentially infectious materials, and either
Discarded, or
For re-useable PPE, cleaned and disinfected according to the manufacturer’s reprocessing instructions and hospital policies.
Hand hygiene should be performed immediately after removal of PPE
Patient Care Equipment
Dedicated medical equipment (preferably disposable, when possible) should be used for the provision of patient care
All non-dedicated, non-disposable medical equipment used for patient care should be cleaned and disinfected according to manufacturer’s instructions and hospital policies
Patient Care Considerations
Limit the use of needles and other sharps as much as possible
Phlebotomy, procedures, and laboratory testing should be limited to the minimum necessary for essential diagnostic evaluation and medical care
All needles and sharps should be handled with extreme care and disposed in puncture-proof, sealed containers
Aerosol Generating Procedures (AGPs)
Avoid AGPs for Ebola HF patients.
If performing AGPs, use a combination of measures to reduce exposures from aerosol-generating procedures when performed on Ebola HF patients.
Visitors should not be present during aerosol-generating procedures.
Limiting the number of HCP present during the procedure to only those essential for patient-care and support.
Conduct the procedures in a private room and ideally in an Airborne Infection Isolation Room (AIIR) when feasible. Room doors should be kept closed during the procedure except when entering or leaving the room, and entry and exit should be minimized during and shortly after the procedure.
HCP should wear gloves, a gown, disposable shoe covers, and either a face shield that fully covers the front and sides of the face or goggles, and respiratory protection that is at least as protective as a NIOSH certified fit-tested N95 filtering facepiece respirator or higher (e.g., powered air purifying respiratory or elastomeric respirator) during aerosol generating procedures.
Conduct environmental surface cleaning following procedures (see section below on environmental infection control).
If re-usable equipment or PPE (e.g. Powered air purifying respirator, elastomeric respirator, etc.) are used, they should be cleaned and disinfected according to manufacturer instructions and hospital policies.
Collection and handling of soiled re-usable respirators must be done by trained individuals using PPE as described above for routine patient care
Although there are limited data available to definitively define a list of AGPs, procedures that are usually included are Bilevel Positive Airway Pressure (BiPAP), bronchoscopy, sputum induction, intubation and extubation, and open suctioning of airways.
Because of the potential risk to individuals reprocessing reusable respirators, disposable filtering face piece respirators are preferred.
Hand Hygiene
HCP should perform hand hygiene frequently, including before and after all patient contact, contact with potentially infectious material, and before putting on and upon removal of PPE, including gloves.
Healthcare facilities should ensure that supplies for performing hand hygiene are available.
Hand hygiene in healthcare settings can be performed by washing with soap and water or using alcohol-based hand rubs. If hands are visibly soiled, use soap and water, not alcohol-based hand rubs.
Facilities should follow safe injection practices as specified under Standard Precautions.
Any injection equipment or parenteral medication container that enters the patient treatment area should be dedicated to that patient and disposed of at the point of use.
Duration of Infection Control Precautions
Duration of precautions should be determined on a case-by-case basis, in conjunction with local, state, and federal health authorities.
Factors that should be considered include, but are not limited to: presence of symptoms related to Ebola HF, date symptoms resolved, other conditions that would require specific precautions (e.g., tuberculosis, Clostridium difficile) and available laboratory information
Monitoring and Management of Potentially Exposed Personnel
Facilities should develop policies for monitoring and management of potentially exposed HCP
Facilities should develop sick leave policies for HCP that are non-punitive, flexible and consistent with public health guidance
Ensure that all HCP, including staff who are not directly employed by the healthcare facility but provide essential daily services, are aware of the sick leave policies.
Persons with percutaneous or mucocutaneous exposures to blood, body fluids, secretions, or excretions from a patient with suspected Ebola HF should
Stop working and immediately wash the affected skin surfaces with soap and water. Mucous membranes (e.g., conjunctiva) should be irrigated with copious amounts of water or eyewash solution
Immediately contact occupational health/supervisor for assessment and access to postexposure management services for all appropriate pathogens (e.g., Human Immunodeficiency Virus, Hepatitis C, etc.)
HCP who develop sudden onset of fever, intense weakness or muscle pains, vomiting, diarrhea, or any signs of hemorrhage after an unprotected exposure (i.e. not wearing recommended PPE at the time of patient contact or through direct contact to blood or body fluids) to a patient with Ebola HF should
Not report to work or should immediately stop working
Notify their supervisor
Seek prompt medical evaluation and testing
Notify local and state health departments
Comply with work exclusion until they are deemed no longer infectious to others
For asymptomatic HCP who had an unprotected exposure (i.e. not wearing recommended PPE at the time of patient contact or through direct contact to blood or body fluids) to a patient with Ebola HF
Should receive medical evaluation and follow-up care including fever monitoring twice daily for 21 days after the last known exposure.
Hospitals should consider policies ensuring twice daily contact with exposed personnel to discuss potential symptoms and document fever checks
May continue to work while receiving twice daily fever checks, based upon hospital policy and discussion with local, state, and federal public health authorities.
Monitoring, Management, and Training of Visitors
Avoid entry of visitors into the patient’s room
Exceptions may be considered on a case by case basis for those who are essential for the patient’s wellbeing.
Establish procedures for monitoring managing and training visitors.
Visits should be scheduled and controlled to allow for:
Screening for Ebola HF (e.g., fever and other symptoms) before entering or upon arrival to the hospital
Evaluating risk to the health of the visitor and ability to comply with precautions
providing instruction, before entry into the patient care area on hand hygiene, limiting surfaces touched, and use of PPE according to the current facility policy while in the patient’s room
Visitor movement within the facility should be restricted to the patient care area and an immediately adjacent waiting area.
Visitors who have been in contact with the Ebola HF patient before and during hospitalization are a possible source of EHF for other patients, visitors, and staff.