Category: Behavior & Population Health Emergencies
The 200x Factor: Why the Newest Veterinary Sedative is Transforming the Drug Crisis

Savage Sisters’ community outreach storefront in the Kensington neighborhood of Philadelphia. (npr.org)
The Invisible Shift: An Introduction
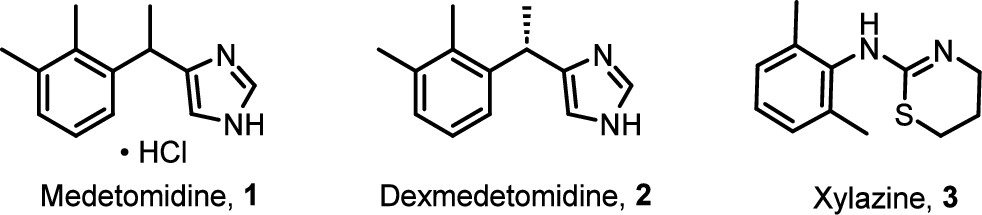
In May 2024, the illicit drug supply in Philadelphia and Chicago underwent a tectonic shift that caught public health systems largely off-guard. For years, the narrative of “Tranq” revolved around xylazine—a veterinary sedative known for leaving users with horrific, necrotic skin ulcers. But a new, stealthier adulterant has arrived: Medetomidine. This isn’t just another additive; it is a pharmacological escalation that mirrors the “China White” (alpha-methylfentanyl) epidemic of the 1970s. Just as China White blindsided the system as a “stealth” fentanyl analog, medetomidine has infiltrated the market under the radar, rendering previous harm-reduction strategies insufficient overnight. This discovery is a game-changer because it signifies a pivot in the supply—moving away from the visible rot of xylazine toward an “invisible” and far more potent cardiovascular killer.
Takeaway 1: The “200x” Potency Leap
Medetomidine represents a massive leap in strength. According to clinical reports, it is between 100 and 200 times more potent than xylazine. While the public is only beginning to understand the dangers of “Tranq,” the illicit market has already evolved into something far more lethal. This extreme potency increases the risk of severe bradycardia (critically slow heart rate), profound hypotension, and respiratory depression. For those on the front lines of harm reduction, this jump in potency means that the “monitoring windows” and supportive care protocols designed for xylazine are now fundamentally inadequate.
“Medetomidine is 100-200 times more potent than xylazine and can cause longer-lasting sedation, low heart rates, and more severe withdrawal symptoms. It is not an opioid but is found in the dope (street opioid) supply.” — Substance Use Philly Report
Takeaway 2: The Bradycardia “Signature”
In recent clusters across Chicago and New Jersey, clinicians have documented a distinct “atypical toxidrome.” Unlike standard opioid overdoses, which primarily shut down the respiratory system, medetomidine leaves a unique cardiovascular footprint. Patients are presenting with heart rates as low as 30–40 beats per minute (bpm)—a level of bradycardia rarely seen with other adulterants. Paradoxically, this is often paired with “hypertensive urgency”—spikes in blood pressure that create a confusing clinical picture for responders used to the “low and slow” profile of heroin.
Clinical Vitals from the ToxIC NOSE Report:
- Heart Rate Range: 34–133 bpm
- Blood Pressure Range: 64/37–170/100 mmHg
Takeaway 3: Why Naloxone Isn’t Enough
The most harrowing aspect for first responders is the “partial response.” Medetomidine is an alpha-2 adrenergic receptor agonist, not an opioid. It induces a deep, heavy sedation by inhibiting noradrenergic neurons in the locus ceruleus—essentially mirroring a state of natural sleep (Stage 2 NREM). This is fundamentally different from the “Mu-receptor” depression of opioids or the “GABAergic” shutdown of benzodiazepines.
When a responder administers naloxone, they may successfully reverse the fentanyl, bringing the patient’s respiratory rate back to normal. However, the patient often remains a “stone-cold” unconscious statue—breathing, but completely unreachable and bradycardic due to the medetomidine. This creates a terrifying clinical limbo where the patient is “saved” from respiratory arrest but remains deeply sedated and cardiac-compromised.
“Because all specimens and samples in this investigation that contained medetomidine also contained natural or synthetic opioids, administering naloxone for all suspected opioid-involved overdoses remains crucial… the effects of medetomidine cannot be reversed with naloxone.” — CDC MMWR Report
Takeaway 4: The “Forbidden” Antidote (Atipamezole)
In the veterinary world, a “cure” for this sedation exists: Atipamezole (Antisedan). It is a highly effective reversal agent used to wake up a bizarrely diverse roster of patients, including okapi, giraffes, red-tailed hawks, koi carp, alligators, and red-eared sliders.
However, Atipamezole is a “forbidden” antidote for humans, presenting a lethal pharmacological catch-22. While it can wake a dog in minutes, administering it to a human who has medetomidine in their system can trigger immediate cardiovascular collapse. This occurs because the drug can cause a sudden drop in blood pressure and profound hypotension while the body is still struggling with reflex bradycardia. We have a way to “wake up” the patient, but the antidote itself could kill them before they open their eyes.
Takeaway 5: The Stealth Takeover of the Supply
The speed at which medetomidine has supplanted xylazine is a testament to the volatility of the illicit market. In Philadelphia, the transition has been near-total in a matter of months. This shift marks a transition from “visible necrosis” (the skin rot associated with xylazine) to “invisible cardiac arrest.” Suppliers are opting for medetomidine likely because its “heavy” sedation profile mimics a more powerful opioid “nod,” even as it silently stresses the user’s heart.
Philadelphia Market Shift (May–November 2024):
- Medetomidine Prevalence: Skyrocketed from 29% to 87%
- Xylazine Prevalence: Plummeted from 97% to 42%
Takeaway 6: The Bizarre Side Effects in Research
Because medetomidine targets the brain’s noradrenergic system so specifically, research has revealed unsettling side effects. In human studies, low doses can actually improve alertness, but the high, uncontrolled doses found on the street likely cause norepinephrine overactivity. This leads to a total collapse of cognitive function; while a user might maintain “selective attention” on a single task, their ability to multitask or respond to their environment vanishes. Furthermore, pharmacological research in monkeys has documented a significant increase in sexual activity following the administration of alpha-2 antagonists, highlighting how deep and unpredictable the neurological impact of these substances truly is.
Conclusion: A New Era of Adulterants
The arrival of medetomidine signals that we have entered a new, more clinical phase of the drug crisis. We are no longer just dealing with opioids; we are managing a supply contaminated with high-potency veterinary anesthetics that require specialized cardiovascular intervention. To survive this, we need a multisector surveillance net—clinicians, toxicology labs, and public health strategists working in a rapid-response loop.
The “Tranq” wounds of yesterday were a warning we could see. The cardiac failures of today are a warning we cannot. As the veterinary-to-street pipeline becomes a permanent fixture of the illicit market, we must ask: Are we prepared for a future where the drug supply evolves faster than our ability to regulate or treat it?
Further Resources

Preventive Interventions in Opioid Addiction: Adaptive Harm Reduction to Reduce Overdoses
In the previous report, we discussed the drastic decrease in mortality seen in South Florida after the establishment of the first needle exchange program in the state.
The very next day, the CDC released preliminary estimates showing a significant rise in all-cause drug mortality nationwide — and particularly mortality secondary to opioid overdose — for many of the same reasons opioid mortality rose over the past decade in Florida:
- the number of people using opioids has risen
- the drugs themselves are becoming more deadly- that is to say, the active components have changed to powerful synthetic opioids.
Over 72,000 people died as a result of an drug overdose in 2017, up 24,000 from just two years prior.

Reducing Mortality in the Opioid Epidemic: What is Miami Doing Differently from the Rest of Florida and the US?
Opioid-related mortality in the United States has soared in the past two decades. A combination of institutional shifts in approaches to pain management, widely publicized unscrupulous marketing and prescribing practices, and increases in the availability and heightened potency of illicit opioids has resulted in such broad loss of life that the US has seen a decrease in the national life expectancy two years in a row. The peak of the HIV/AIDS crisis resulted in a one-year drop in life expectancy in 1993, but a multi-year drop has not been seen since 1963, with the occurrence of the Hong Kong H3N2 influenza pandemic.
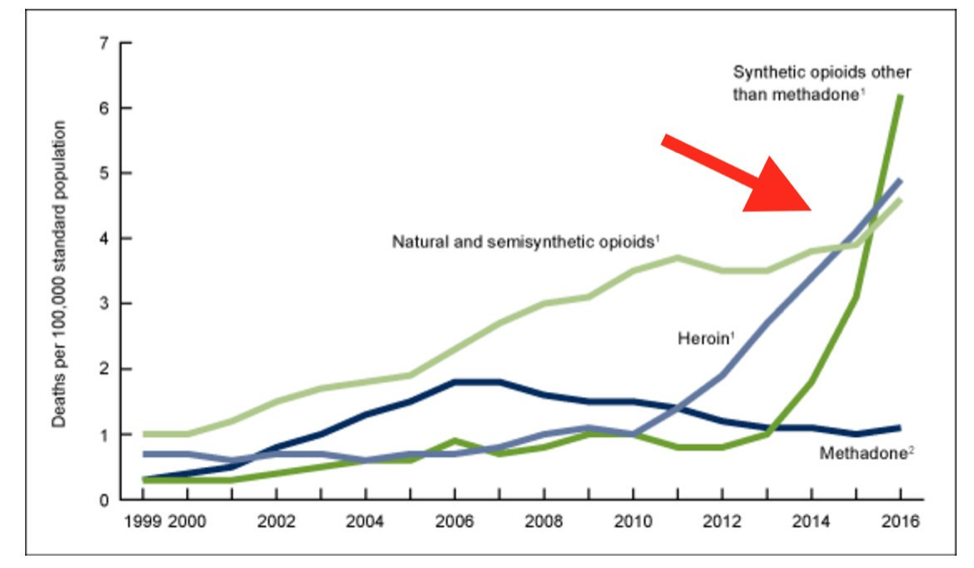
Age-adjusted drug overdose death rates by opioid category United States 1999-2016

Gun Violence: A Public Health Epidemic?

Image by Flickr User Cerebralzero
This is not a discussion about the 2nd Amendment or about the “right to bear arms.” This is an analysis of the public health impact of violence and scientific strategies to reduce injuries and deaths from firearms.
Georges Benjamin, the Executive Director of the American Public Health Association, believes we have a gun violence “epidemic.” With over 30,000 people in America dying annually from firearm-related violence, he believes “we should track it, find the root causes, use science to find research gaps, create policy solutions and use mass public education campaigns to eradicate the threat.” He argues that scientific methods were used in the face of increasing deaths from automobile accidents to great success and that scientists should be allowed to study gun violence just as they did for Ebola.
America’s Latest Battlefront in the War on Drugs: Heroin

(Courtesy of emcdda.europa.eu)
Close your eyes and picture a heroin addict. Chances are you’re thinking of a young, uneducated, low-income youth with a significant criminal background. The face of heroin in America is changing and likely doesn’t look like whom you would expect. Communities across the nation are facing a staggering epidemic of heroin abuse. New York City had more deaths from heroin overdose in 2014 than in any year since 2003, in 2013 420 of 782 fatal drug overdoses in the city were due to this increasingly popular drug.
Quarantine: Ethical & Legal Battle for Human Rights during Public Health Emergencies
As the Ebola Epidemic of 2014 continues, some officials are calling upon a centuries-old tactic to combat the disease: medical quarantine. In an effort that began on October 24th, New York and New Jersey state officials instituted a mandatory 21-day quarantine on all medical personnel returning from volunteer efforts to combat the disease in West Africa.

No Standard Protocols
While some states are embracing the idea and implementing quarantines of their own, other state and national officials are denouncing them. Medecins Sans Frontieres (MSF), the main humanitarian group coordinating volunteer efforts in Africa also denounced the quarantines:
There are other ways to adequately address both public anxiety and health imperatives, and the response to Ebola must not be guided primarily by panic in countries not overly affected by the epidemic,” said Sophie Delaunay, executive director of MSF-USA. “Any regulation not based on scientific medical grounds, which would isolate healthy aid workers, will very likely serve as a disincentive to others to combat the epidemic at its source, in West Africa.
International MSF staff members commit to burdensome four-to-six week assignments in the Ebola affected countries. The risk of being quarantined for 21 days upon completion of their work has already prompted some people to reduce their length of time in the field. Others will be less inclined to volunteer in the first place. This will present significant operational disruptions at the field level for MSF and other organizations, and lead to an overall shortage of desperately needed health workers, precisely when the Ebola outbreak is as out of control as ever.
Mental Health Preparedness: Psychological Protection Prior to a Disaster
This is the second in a three-part series on post traumatic stress disorder following disasters. Part One, PTSD in Emergency Workers, can be found here.
General Public at Risk
Over 2/3 of the general population will experience some significant traumatic event in their lifetime, and 1/5 of Americans will undergo such an event in any year. One review of the literature found that the prevalence of PTSD in direct victims can range from 30-40%, in rescue workers 10-20%, and 5-10% in the general population.

Public Health Crisis on the US Border: Health & Immigration Policies Collide
Children Escaping Violence & Poverty
Over 50,000 undocumented children (UAC) have entered the United States through the Southwestern border in the last 8 months, creating what some a calling a humanitarian crisis. As many as 90,000 children are expected to enter the country by the end of the year.

Many children are being sent to the United States alone without any adult supervision by family members hoping that by entering the United States their children will be spared the harsh realities of gang violence, drug cartels and civil unrest in their home countries. Categorized as Unaccompanied Alien Children (UAC), these children hail mostly from Mexico, Guatemala, El Salvador, Honduras and Ecuador.
PTSD in Emergency Workers
This is the first of a series of posts which will cover post-traumatic stress disorder (PTSD).
EMTs, Paramedics, Fire Fighters, Police Officers, Emergency Department Personnel. These brave individuals serve to protect, to save, and to heal us in times of our greatest need. Aid workers are dispatched around the world to respond to natural and man-made disasters such as earthquakes, hurricanes, and war. Just as our nation’s soldiers and veterans battle the effects of post-traumatic stress disorder (PTSD), so do our first responders. Worldwide 1 in 10 emergency workers have PTSD. Ambulance personnel are the hardest hit, with over 1 in 5 ambulance personnel meeting criteria.

Image courtesy of the LA Times
