PTSD in Emergency Workers
This is the first of a series of posts which will cover post-traumatic stress disorder (PTSD).
EMTs, Paramedics, Fire Fighters, Police Officers, Emergency Department Personnel. These brave individuals serve to protect, to save, and to heal us in times of our greatest need. Aid workers are dispatched around the world to respond to natural and man-made disasters such as earthquakes, hurricanes, and war. Just as our nation’s soldiers and veterans battle the effects of post-traumatic stress disorder (PTSD), so do our first responders. Worldwide 1 in 10 emergency workers have PTSD. Ambulance personnel are the hardest hit, with over 1 in 5 ambulance personnel meeting criteria.

Image courtesy of the LA Times
Definition and Prevalence
In the newest version of DSM, the DSM-V, published by the American Psychiatric Association, PTSD was moved from being characterized as an anxiety disorder, to a new category of Trauma- and Stress-or-Related Disorders. Per the new definition, the PTSD trigger must be an exposure to actual or threatened death, serious injury or sexual violation. The exposure must result from one or more of the following scenarios, in which the individual:
- directly experiences the traumatic event
- witnesses the traumatic even in person
- learns that the traumatic event occurred to a close family member or close friend (with the actual or threatened death being either violent or accidental); or
- experiences first-hand repeated or extreme exposure to aversive details of the traumatic event (not through media, pictures, television or movies unless work- related).
Additionally, the disturbance must cause clinically significant distress or impairment in the individual’s social interactions, capacity to work or other important areas of functioning.
Emergency department nurses and physicians are not immune to the effects of PTSD. A survey of Emergency Department nurses found that only 13% reported no confrontation with a traumatic event in the last 6 months, 15% reported only one event, 32% two or three events, 23%, four or five events and 17% reported six events or more. The respondents found that emergencies involving young children and physical trauma to be the most emotionally taxing.
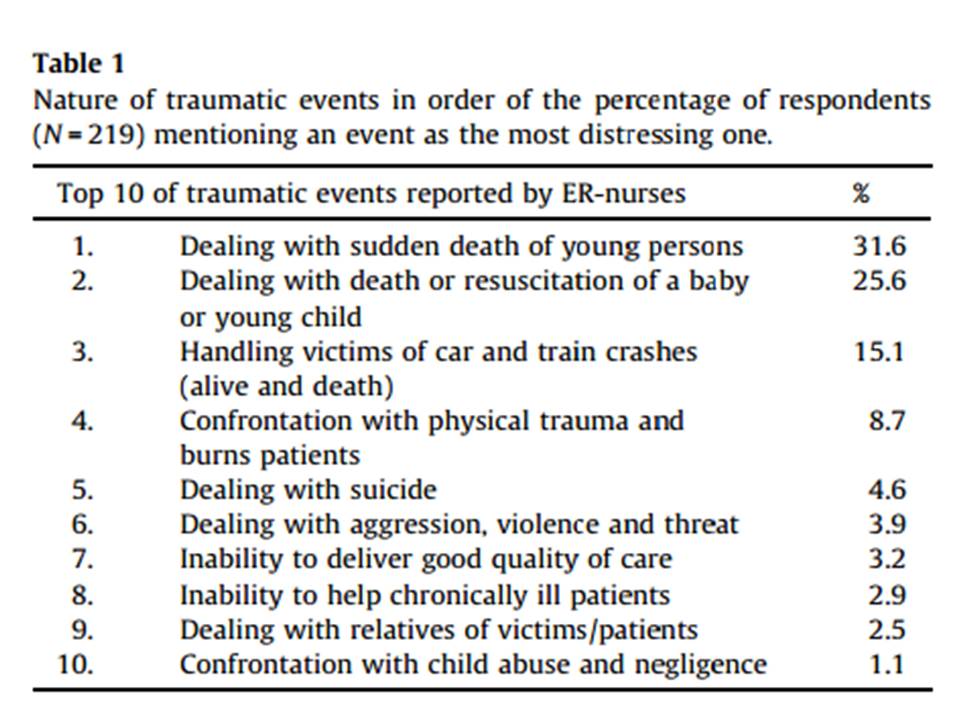
Nature of traumatic events in order of the percentage of Emergency Nurses
(N = 219) mentioning an event as the most distressing one.
Another study showed that while ED nurses have the symptoms of PTSD, they do not often seek professional help or attend critical incident debriefs after upsetting events.
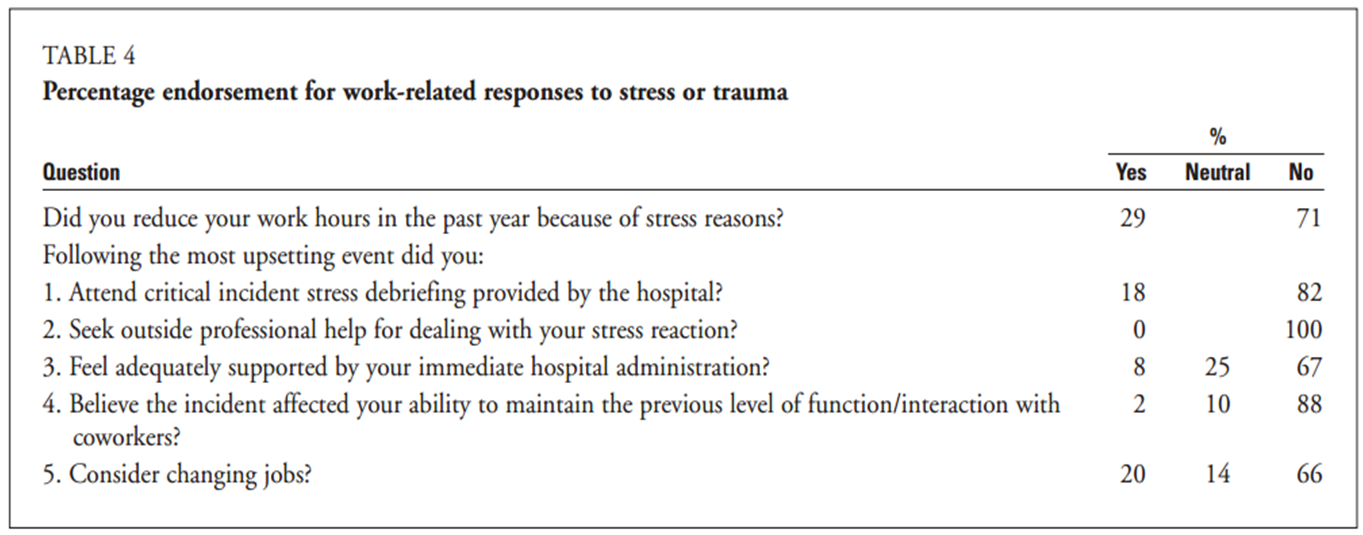
Percentage ED Nurse endorsement for work-related responses to stress or trauma
Physicians, too, experience the effects of PTSD. A survey of Emergency Medicine residents in one hospital in 2003 found that nearly 12% met criteria for PTSD, 30% had one or more symptoms of each of three categories (re-experience, avoiding, increased arousal), and the longer a resident had worked in the ED, the more likely they were to have positive symptoms.
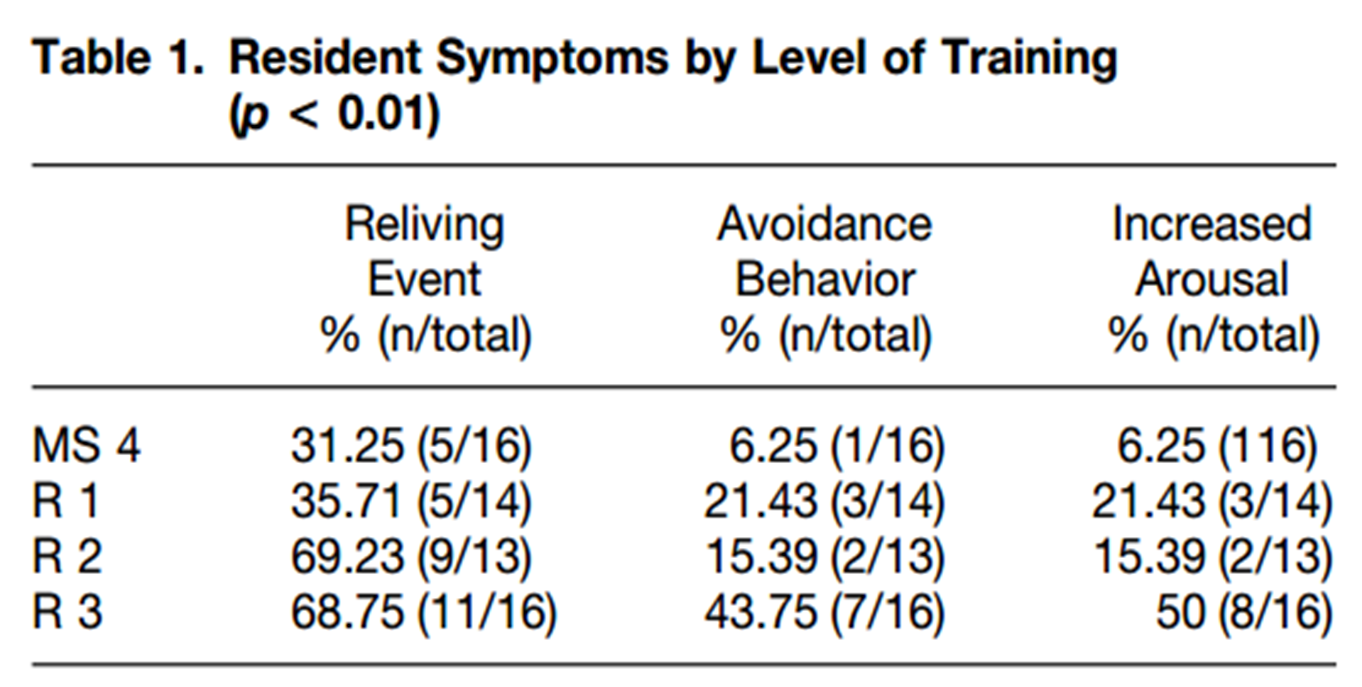
EM Resident Symptoms of PTSD
This special report by Anne Scheck in Emergency Medicine News further highlights data on PTSD among physicians and response workers. Ms. Scheck notes that having an outlet to discuss distressing events has been shown to mitigate the effects of PTSD, but often providers do not take advantage of these resources.
I visited MIT a few months after the horrific killing of a police officer at my alma mater. It was the MIT Police Department and MIT-EMS who were first on scene and who rushed to the aid of their close friend. As a prior member of MIT-EMS I had been close with many members of both services, and visited one officer to offer my condolences. We sat across each other at a small table in his office, his suit was as crisp as always and he sat up straight with his usual air of confidence. Within minutes, however, he was in tears. He spoke of the pain he felt, and that felt by his brothers and sisters in the service, and of the mental health resources that had been brought in to support the officers during the troubling time. When asked if he had taken advantage of these resources, he laughed slightly and said ‘No, but I should’.
Dr. Edwin Leap describes this cultural resistance to seek help among physicians.
It makes sense, doesn’t it? If you stand next to enough bleeding people, you get bloody. If you breathe the air of patients with the flu, you get the flu. If you spend enough time around people who have experienced terrible, life-altering events, the emotions can stick to you, especially when your job is to hear the story, view the wounds, fix the wounds, and try to bring order and safety to the victim.
The odd thing is, we tend to be sympathetic to those with the disorder. We believe their stories whether they involve mortar attacks, IEDs, child abuse, or animal attacks. But we seem unwilling to accept that it might be happening to us, the White Knights of medicine (and nursing and EMS) who see the worst things on the front lines.
Maybe we don’t like to embrace our humanity or our vulnerability. Perhaps we developed the incorrect belief that a mental illness is a moral failure or that admitting to one might adversely affect our careers. I suppose it could be because we get paid to expose our bodies and minds to terrible events. If it’s our job and we’re paid, what right do we have to be wounded? Shouldn’t we just suck it up?
Emergency Workers: “Protect thyself”
So what can be done?
The first step is to recognize the signs and symptoms of PTSD. Per the CDC & NIOSH, these include:
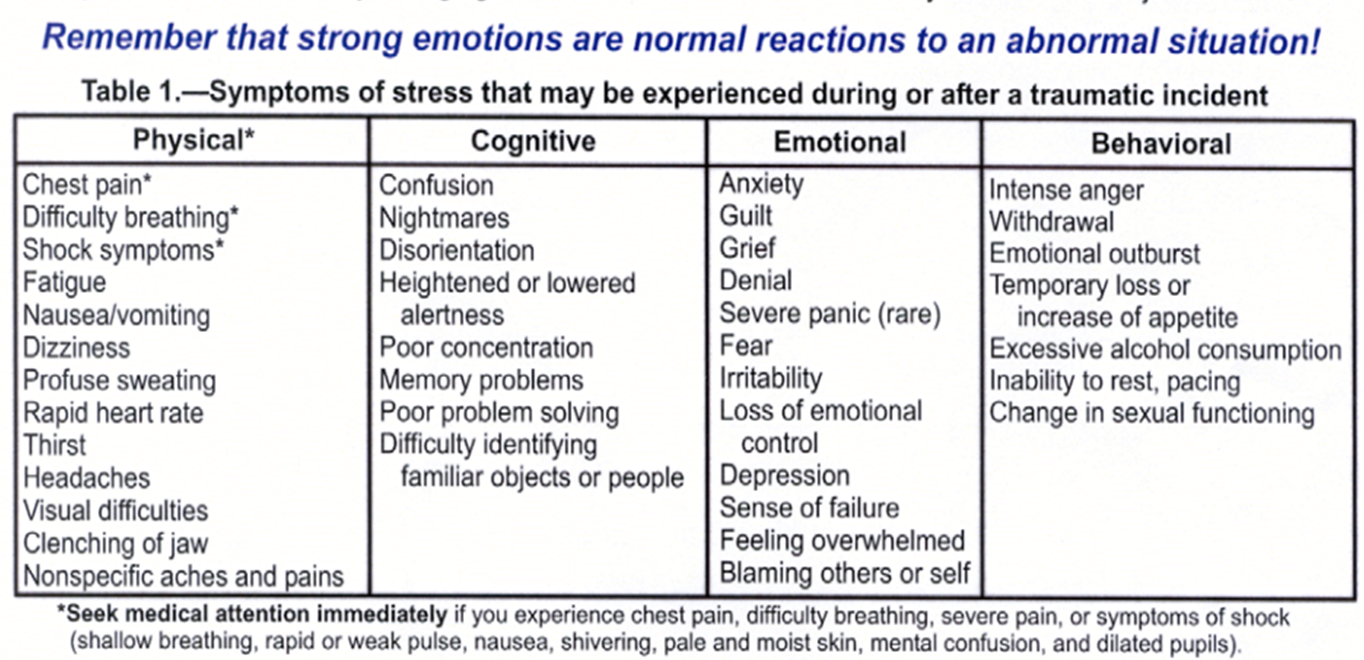
Symptoms of PTSD
During the emergent event, it is recommended that rescue workers:
- Pace themselves
- Watch out for one another, especially in hazardous environments, and be conscious of those who are exhausted or stressed
- Take frequent rest breaks – when possible away from the work area
- Eat and sleep regularly, drink plenty of fluids, & increase intake of complex carbs
- Recognize and accept what cannot be changed (chain of command, organizational structure, etc)
- Utilize formal mental health support provided by employers
- Follow their own time table on when to discuss the experience with friends and family members.
- Give themselves permission to feel rotten and know that recurring thoughts, dreams, or flashbacks are normal and should decrease with time
After the event, it is recommended that rescue workers:
- Reach out to family, spiritual, and community supporters
- Consider keeping a journal
- Avoid making any big life decisions for a while, but make as many daily decisions as possible to maintain a feeling of control
- Spend time alone or with others doing enjoyable tasks
- Know that it is normal to feel particularly fearful for family and loved ones
- Remember that ‘getting back to normal’ takes time and that recovers is not a straight path.
- Appreciate a sense of humor in yourself and others. It is ok to laugh
- Avoid overuse of drugs or alcohol and get plenty of rest, exercise and healthy and regular meals
Have you or your co-workers experienced PTSD? Does your institution or employer provide resources and support for those experiencing symptoms? If so, are they utilized? Leave a comment below!
 This post is dedicated to the family of fallen Officer Sean Collier, and my dear friends at MIT PD and MIT-EMS. Forever Boston Strong. Forever MIT Strong. Forever Collier Strong.
This post is dedicated to the family of fallen Officer Sean Collier, and my dear friends at MIT PD and MIT-EMS. Forever Boston Strong. Forever MIT Strong. Forever Collier Strong.
Report written by Vidya Eswaran

I worked Security in the ED for twenty yrs. I can remember so many deaths and …. so much anguish. I remember a car shot up, dead man in the back seat, 15yr old with the back of his head blown off, and the list goes on. Retired now but forgetting is another thing. Your article hit home.
Thank you for your comment, Charles, and thank you for the work you did in your ED. This is a subject about which we need to increase awareness and take substantial steps in order to help each other.
I think this is an extremely important topic. Mental health, particularly PTSD with emergency response workers is something that needs to be recognized and we need to begin following through with appropriate treatment.