Anthrax on the Loose
CDC Employees Exposed to Deadly Bacteria
On June 19, 2014, the CDC announced that about 75 Atlanta based staff may have been exposed to life Bacillus anthracis, or anthrax, the deadly bacterial spores which were used as weapons of biological terrorism is 2001. The number of exposed staff has since been increased to 84, with 7 at increased risk because they had more direct exposure to the spores.

Bacillus anthracis Picture courtesty of PBS

Responders to CDC Anthrax Release Courtesy of BBC
B.anthracis is a spore-forming, gram positive bacillus, which when inhaled carries a high mortality. The spores can enter the body cutaneously, enterally, via injection or via inhalation. Patients with inhalation anthrax will present with fever, chills, headache, chest pain, cough and difficulty breathing, and will require hospitalization even though they may not appear critically ill. These patients are susceptible to sudden decline and hemodynamic monitoring should be initiated. Chest CT and CXR will show characteristically widened mediastinum and pleural effusions.


Anthrax CXR

It is believed that the exposure occurred when spores at the Roybal campus biosafety level (BSL) 3 labs were inadequately inactivated (stored in chemical inactivating medium for 24 hours instead of the 48 protocol required). These spores were then transferred to two different BSL-2 laboratories which were developing new methods of detection, and where staff handled the bacteria-containing test tubes wearing little more than glows, gowns and goggles. Within a week scientists at the original lab noticed that samples of the bacteria left in an incubator were growing live anthrax. This same facility, also known as Building 18, was found to have a potentially dangerous airflow leak in February of 2012.

CDC Building 18
Laboratory-Acquired Infections
Per the U.S. Bureau of Labor Statistics, in 2008, 500,000 people worked in human and animal diagnostic laboratories, of which 328,000 were medical lab technicians and technologists (likely with greatest risk of exposure to infectious agents). Over 40% of laboratory-acquired infections (LAI) are due to bacteria, and Hepatitis B is the most common viral source of LAI. Per the CDC, the five most common routes of LAI are:
- Parental inoculations with syringe needles or other contaminated sharps
- Spills and splashes onto skin and mucous membranes
- Ingestion or exposure through mouth pipetting (my note: who on earth is still mouth pipetting??) or touching mouth or eyes with fingers or contaminated objects
- Animal bites and scratches (research laboratories or activities)
- Inhalation of infectious aerosols
The last route, however, accounts of 80% of all LAIs and are, unfortunately, the most difficult to track In fact, the probably sources of LAIs are apparent in only 50% of all cases.
To mitigate against this danger, laboratory directors are tasked with the responsibility for
- Establishing and enforcing a culture of safety within the laboratory
- Identifying as many hazards as possible and specifying practices and procedures that will minimize or eliminate those hazards
- Ensuring that all personnel are instructed in and engaged in performing risk assessments and demonstrating that they can identify laboratory hazards in their individual work environments
- Ensuring that all personnel are trained and competent in the standard practices and techniques that minimize identified workplace hazards
- Providing an avenue for personnel to identify hazards and to present risk-mitigation strategies to management, and
- Educating clinicians and nurses about safe specimen procurement and transport to ensure their safety and that of the laboratory personnel who receive the clinical samples
The World Organization for Animal Health (OIE) and the CDC/NIH have developed a classification system for laboratories which handle dangerous specimen.


Bio-safety Recommendations
For anthrax in particular, NIOSH recommends workers don powered air-purifying respirators with full facepiece and HEPA filters, disposable protective clothing with integral hood and booties and disposable gloves.
The entire handbook, Biosafety in Microbiological and Biomedical Laboratories, 5th Edition can be found here.
While release of anthrax from laboratories is certainly of major concern, the CDC has also created plans to be enacted in the event of its release as a bioterrorist agent. In such an event, the CDC and its partners would respond by:
- Sending samples through the Laboratory Response Network
- Continuing to test samples to learn more about the strain of anthrax
- Deploying field staff to talk to patients and learn more about how they were exposed
- Shipping out medicine and supplies from the Strategic National Stockpile (SNS) to local Points of Dispensing (PODs_
- Provide guidance to clinicians, health departments and other partners on how to respond
- Communicating life-saving information to the public
No validated methods for monitoring anthrax exposure exist, and the CDC recommends 6 0days of antibiotic prophylaxis after exposure. Additionally the CDC recommends anthrax vaccine BioThrax ™ for any workers making repeated entries into known contaminated areas.
Recommendations for medical program components to prevent anthrax among remediation workers
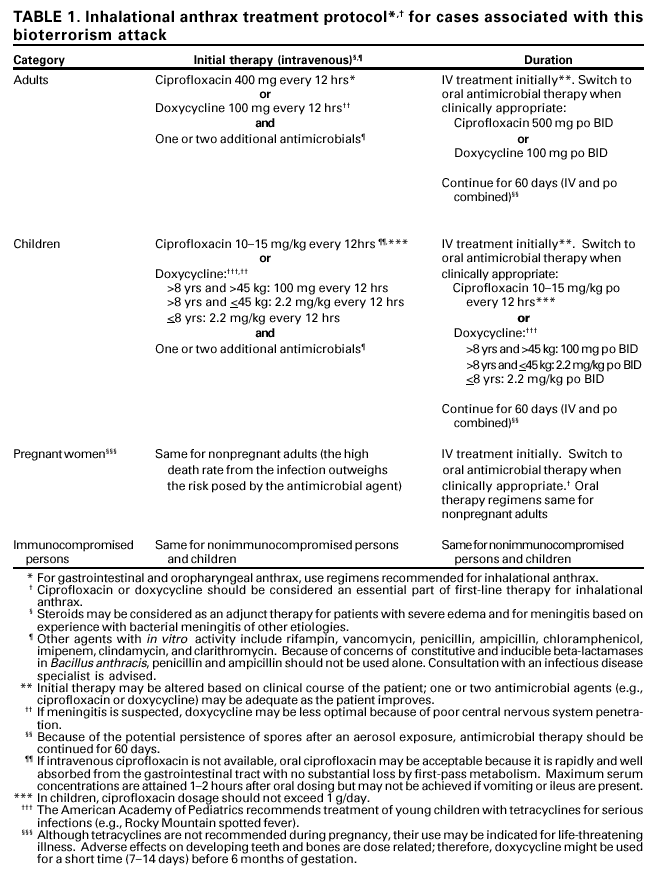
Inhalational anthrax treatment protocol
A facility should be closed if an inhalation anthrax case is detected and the site is the probable source, if there is a known, or strong suspicion of aerosolization of anthrax within the facility, of if needed to be closed by law enforcement agencies in a criminal investigation.
In the wake of this latest breach of safety standards at the CDC, investigations will need to be made into whether more stringent protocols are needed to keep Americans safe from deadly disease.
Report Written by Vidya Eswaran
